
Hey Doc, Mr. Jones in R4 is starting to sundown and keeps trying to get out of bed, do you have anything to sedate him? You look into R4 and Mr. Jones is pulling off his pulse ox and yelling at the tech, he definitely needs something to calm him down. However, Mr. Jones is 83 and is being admitted for CHF exacerbation on 5L NC, you also remember his ECG looking funny so you pull it up again. Oh yeah, he has a QTc of 509…that makes sedating him a bit more difficult. You think through your go-to list of medications…he is already on oxygen and hypoxic so you want to be careful about causing too much CNS depression with benzos, and his QTc is long so can you safely give him an antipsychotic? You vaguely remember that haldol seemed to be safe-ish, but haven’t we all heard a horror story of someone going into torsades? Are there any other options?
Well, after this episode of The Cheese you will be able to safely and confidently pick the antipsychotic medication of choice!
Antipsychotic Selection and Risk of QTc Prolongation
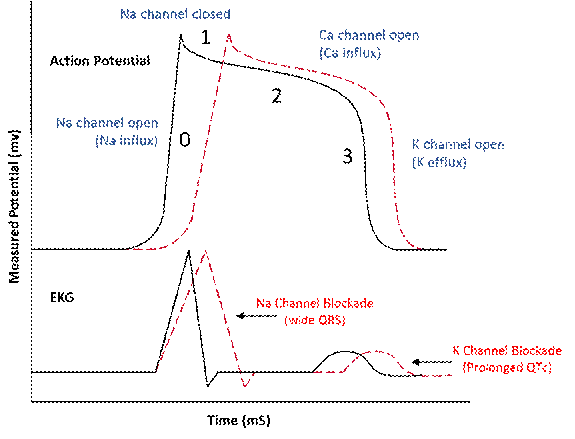
QTc prolongation is a clinically important adverse effect associated with antipsychotic medications because it increases the risk of torsades de pointes and sudden cardiac death. Drug-induced QT prolongation typically occurs through blockade of cardiac potassium channels (particularly the IKr current mediated by the hERG channel), which delays ventricular repolarization (Figure 1).
Evidence From Clinical Studies
A randomized study evaluated QTc changes associated with several commonly used antipsychotics including haloperidol, thioridazine, ziprasidone, quetiapine, olanzapine, and risperidone (Ray, 2009). The investigators found that even though all agents produced measurable QTc prolongation, the magnitude differed substantially between medications. Thioridazine produced the largest mean QTc increase. In contrast, olanzapine and haloperidol were associated with relatively small mean QTc changes. These findings reinforce earlier reviews which reported wide variability in QT-prolonging effects across antipsychotics (Zareba, 2003). Typical increases in QTc ranged from approximately 4–6 ms with agents such as haloperidol or olanzapine to up to ~35 ms with thioridazine, highlighting diversity in cardiotoxic potential across drugs in this class. Furthermore, they concluded that arrhythmias caused by a QT-prolonging drug occur infrequently, and usually multiple factors are needed to precipitate such an event including a combination of two or more drugs affecting the same pathway, hypokalemia, and possibly genetic predisposition.
Relative QTc Risk Among Antipsychotics
Together, the studies suggest a hierarchy of QTc risk:
Higher QTc prolongation risk
Thioridazine
Moderate risk
Ziprasidone
Quetiapine
Risperidone
Lower risk
Olanzapine
Haloperidol
This stratification aligns with mechanistic differences in potassium channel blockade. Certain atypical antipsychotics, including quetiapine, risperidone, and olanzapine, showed greater selectivity for D2 and 5-HT2A receptors when compared to IKr receptors, correlating with lower impact on the QTc interval.
A more recent study from 2024 had similar findings to the two previously mentioned papers (Melo, 2024). This paper summarized the current literature surrounding antipsychotics and QTc prolongation (Figure 2). They noted that ziprasidone carried the highest risk of torsades de pointes and olanzapine had one of the lowest risks.
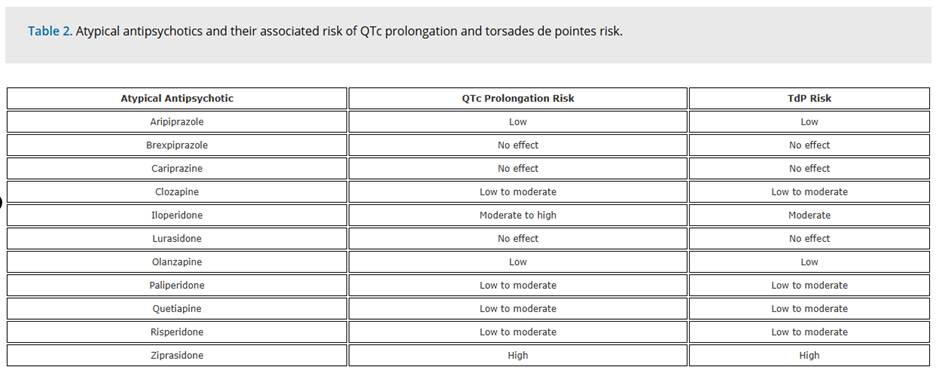
Figure 2. Agent specific risks (Melo et al)
Clinical Context and Risk Modifiers
All three papers emphasize that QTc prolongation rarely occurs in isolation and is usually influenced by multiple patient-specific risk factors. These include electrolyte abnormalities (particularly hypokalemia), drug interactions affecting metabolism, structural heart disease, advanced age, and polypharmacy with other QT-prolonging medications. Genetic predisposition may also contribute to individual susceptibility.
Conclusion
Olanzapine carries one of the lowest risks of QTc prolongation and torsades de pointes. In the case of Mr. Jones, my go to would be olanzapine given it is available in an intramuscular formulation, and it is relatively low risk. There is only one published case report of torsades de pointes after olanzapine use, thus I would probably stick with olanzapine in patients with a borderline or prolonged QTc if possible (Huang, 2014). Furthermore, another study looked at the effects of intramuscular olanzapine in acute agitation with schizophrenia or dementia in the emergency department and found that there was no significant QTc prolongation with olanzapine use (Lindborg, 2003). While there are case reports describing torsade de pointes and sudden cardiac death following haloperidol administration, we have been using it for decades, and it is still generally considered a lower-risk agent. There very well may be clinical situations where its use is appropriate or necessary given that it is easier to prepare or available quicker (i.e. in a pyxis). At the end of the day it’s all about the right drug, in the right dose, for the right patient!
Citations
Ray WA, Chung CP, Murray KT, Hall K, Stein CM. Atypical antipsychotic drugs and the risk of sudden cardiac death. N Engl J Med. 2009 Jan 15;360(3):225-35. doi: 10.1056/NEJMoa0806994. Erratum in: N Engl J Med. 2009 Oct 29;361(18):1814. PMID: 19144938; PMCID: PMC2713724.
Zareba W, Lin DA. Antipsychotic drugs and QT interval prolongation. Psychiatr Q. 2003 Fall;74(3):291-306. doi: 10.1023/a:1024122706337. PMID: 12918603.
Melo L, Pillai A, Kompella R, Patail H, Aronow WS. An Updated Safety Review of the Relationship Between Atypical Antipsychotic Drugs, the QTc Interval and Torsades de Pointe As: Implications for Clinical Use. Expert Opin Drug Saf. 2024 Sep;23(9):1127-1134. doi: 10.1080/14740338.2024.2392002. Epub 2024 Aug 13. PMID: 39126643.
Huang G, Fu Q, Xu J. Potential torsades de pointes triggered by hypokalemia related to olanzapine in a patient with implantable cardioverter-defibrillator. J Clin Psychopharmacol. 2014 Oct;34(5):651-2.
Lindborg SR, Beasley CM, Alaka K, Taylor CC. Effects of intramuscular olanzapine vs. haloperidol and placebo on QTc intervals in acutely agitated patients. Psychiatry Res. 2003 Jul 15;119(1-2):113-23.
Authored by Taylor Wahrenbrock MD, Joanne Rutsolias PharmD, & Eric Leser MD