
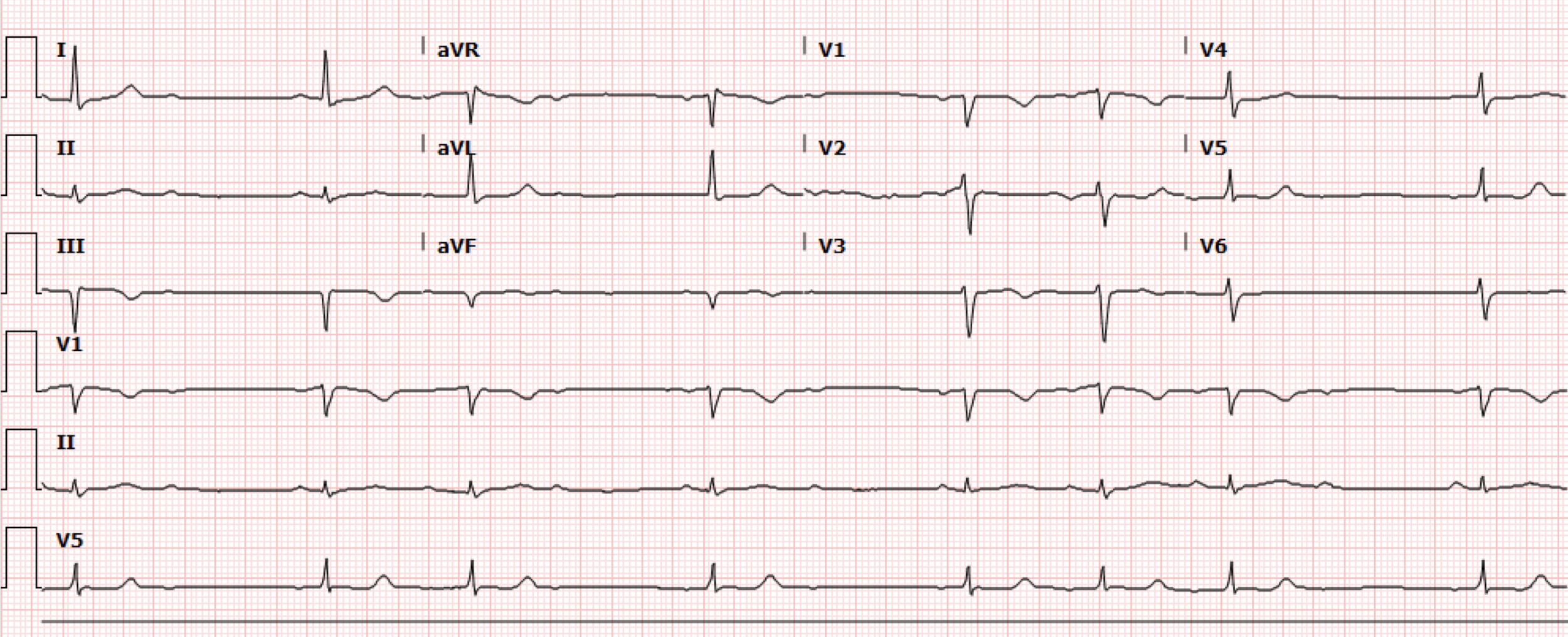
A 59-year-old male with no known medical history presents to the emergency department with complaints of chest pain and shortness of breath for one week. The chest pain and shortness of breath is exertional and acutely worsened on the day of presentation which prompted the ED visit. Initial vital signs notable for BP 106/87, HR 45, RR 18 and oxygen saturation 98% on room air. The patient’s initial EKG (Figure 1) is shown.
Interpretation: Rate: 45 bpm; Rhythm: sinus rhythm Axis: left axis deviation (I: pos, II: pos, aVF: neg Intervals: PR: variable length, gradually prolonging until one QRS dropped ; QRS: 113; QTc: 436–normal; P-Waves: present QRS Complex: dropped complex with variable pattern; ST Segment/T-waves: no ST elevation, T wave inversions lead III, deep Q waves in lead III and aVF
Transcutaneous pacing pads were subsequently placed on the patient. The initial labs were notable for a high sensitivity troponin elevation to 2,337 and BNP of 1214. Bedside POCUS performed showed possible inferior region wall abnormality. And on close review of the EKG, the pattern is consistent with a Mobitz Type I/Wenckebach morphology. Cardiology was consulted due to concern for a new AV block in the setting of an OMI. The patient was taken to the cath lab urgently and found to have 100% proximal RCA occlusion and 90% LAD occlusion.
Discussion:
Normal heart conduction begins at the SA node, is then conducted through the atrium to the AV node, down through the bundle of His, followed by distribution through the right and left bundle branches, and finally through the purkinje fibers to left and right ventricles. Any disruption in this electrical circuit can result in pathologic and/or symptomatic bradycardia.
Symptomatic bradycardia indicates the presence of bradycardia (HR<60) with symptoms that can include: syncope, lightheadedness, chest pain, fatigue. A basic algorithm (Figure 2) for treatment of symptomatic algorithm is as follows:
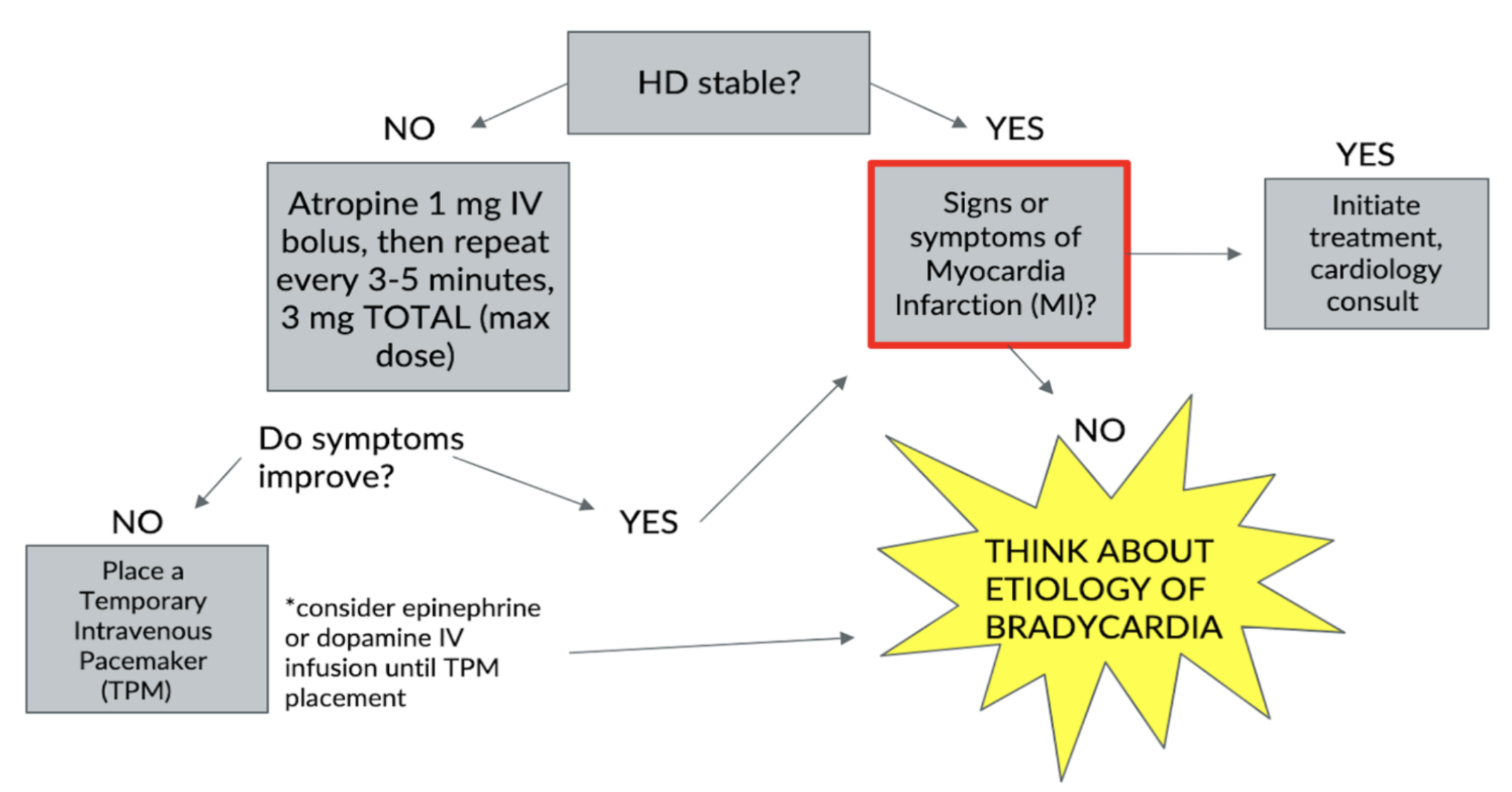
Figure 2. Symptomatic bradycardia algorithm (Image from: https://www.nuemblog.com/blog/symptomatic-bradycardia)
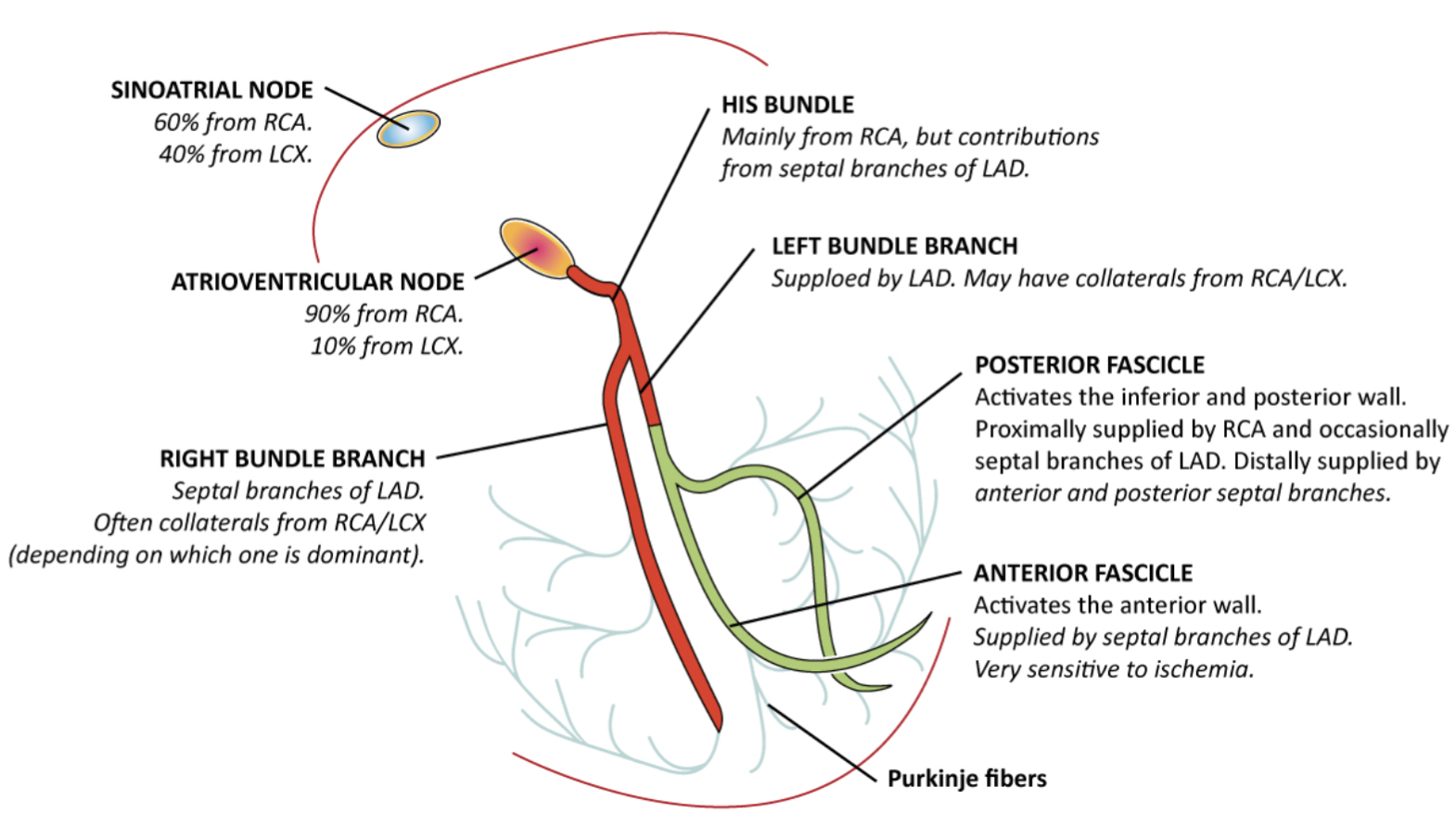
Figure 3. Vascular supply of the cardiac conduction system (Image from: https://ecgwaves.com/topic/conduction-defects-myocardial-ischemia-infarction/)
Bradyarrhythmias occur in about 15-25% of patients with an acute myocardial infarction. To understand this relationship lets review the vascular supply of the conduction system (Figure 3). The SA node receives its blood supply from the right coronary artery (RCA) in approximately 60% of individuals, while the left circumflex artery (LCx) supplies the remaining 40%. The atrioventricular (AV) node is supplied by the RCA in about 90% of patients, with the LCx accounting for the other 10%. The bundle of his is mostly supplied by the RCA with minor supply from the LAD.
In the case of RCA occlusion, seen in inferior, inferolateral and inferoposterior myocardial ischemia, ischemia affects supply to SA node, AV node and Bundle of His which can then depress nodal automaticity and slow AV conduction. Therefore this can present as a spectrum of rhythms that includes but not limited to: sinus bradycardia, sinus arrest, junctional rhythms, idioventricular block, AV conduction blocks such as first degree AV block, Mobitz I and complete heart block. Sinus bradycardia accounts for the majority (~30-40%) of bradycardic rhythms in acute ischemia. AV conduction blocks also frequently occur in bradyarrhythmias in acute ischemia. Mobitz I compared to Mobitz II particularly occurs more frequently in RCA occlusion as the AV node tend to be more resilient to complete ischemia than the His-purkinje system, which typically causes Mobitz II AV block.
Therefore a “fatigue-type” conduction delay occurs where conduction slows beat to beat (characteristic progressive PR interval prolongation) and eventually one impulse fails (dropped QRS) (Figure 4). In addition to the direct ischemic effects, inferior wall infarction from RCA occlusion frequently triggers the Bezold–Jarisch reflex—a neurocardiogenic response in which ventricular mechanoreceptors activate vagal pathways, increasing parasympathetic tone. The AV node, highly sensitive to this vagal influence, responds with slowed conduction, contributing to sinus bradycardia and progressive PR interval prolongation.

Figure 4: V5 lead in our patient’s EKG demonstrating the classic PR prolongation resulting in a non-conducted P wave and a dropped beat
Treatment for hemodynamically stable Mobitz I AV block in the setting of acute ischemia in the emergency department, includes urgent cardiology consult and cath lab activation. Patients should be continuously monitored and have transcutaneous pacer pads placed in the event of clinical deterioration. Atropine 1-3mg has been found to be helpful in 70-80% of ACS patients and leads to increased heart rate. Bradyarrhythmias particularly in inferior OMI are transient and ultimately do not require a pacemaker placement and resolve after prompt revascularization.
Take home-points:
Acute myocardial ischemia is a common cause of symptomatic bradycardia and must be ruled out.
RCA occlusion which commonly presents as inferior OMI, can disrupt SA node, AV node and bundle of His conduction which leads to bradyarrhythmias such as Mobitz I(Wenckebach) such as in our patient above.
Management of bradycardia during acute myocardial ischemia involves prompt cardiology consultation and definitive treatment with coronary revascularization. Atropine may be administered as a temporary measure, and most patients respond favorably to it.
Sources:
Zimetbaum, Peter. “Conduction Abnormalities after Myocardial Infarction.” UpToDate, 8 Sept. 2025, www.uptodate.com/contents/conduction-abnormalities-after-myocardial-infarction#H14.
Trappe H. J. (2010). Tachyarrhythmias, bradyarrhythmias and acute coronary syndromes. Journal of emergencies, trauma, and shock, 3(2), 137–142. https://doi.org/10.4103/0974-2700.62112
“Symptomatic Bradycardia: Considering the Differential.” NUEM Blog, NUEM Blog, 17 June 2024, www.nuemblog.com/blog/symptomatic-bradycardia.
Authored by Abish Kharel MD and Ari Edelheit MD