
The patient is a 52-year-old female, with a past medical history of hypertension, congestive heart failure, atrial fibrillation on rivaroxaban, and type 2 diabetes who is presenting with palpitations and shortness of breath for two days. Episodes last 1-3 minutes at a time before resolving. She has a history of similar symptoms the month prior, for which her cardiologist recommended an ablation in the future.
Vital Signs: HR: 101, BP: 101/18, RR: 18, O2 100% on RA, Temp 37C
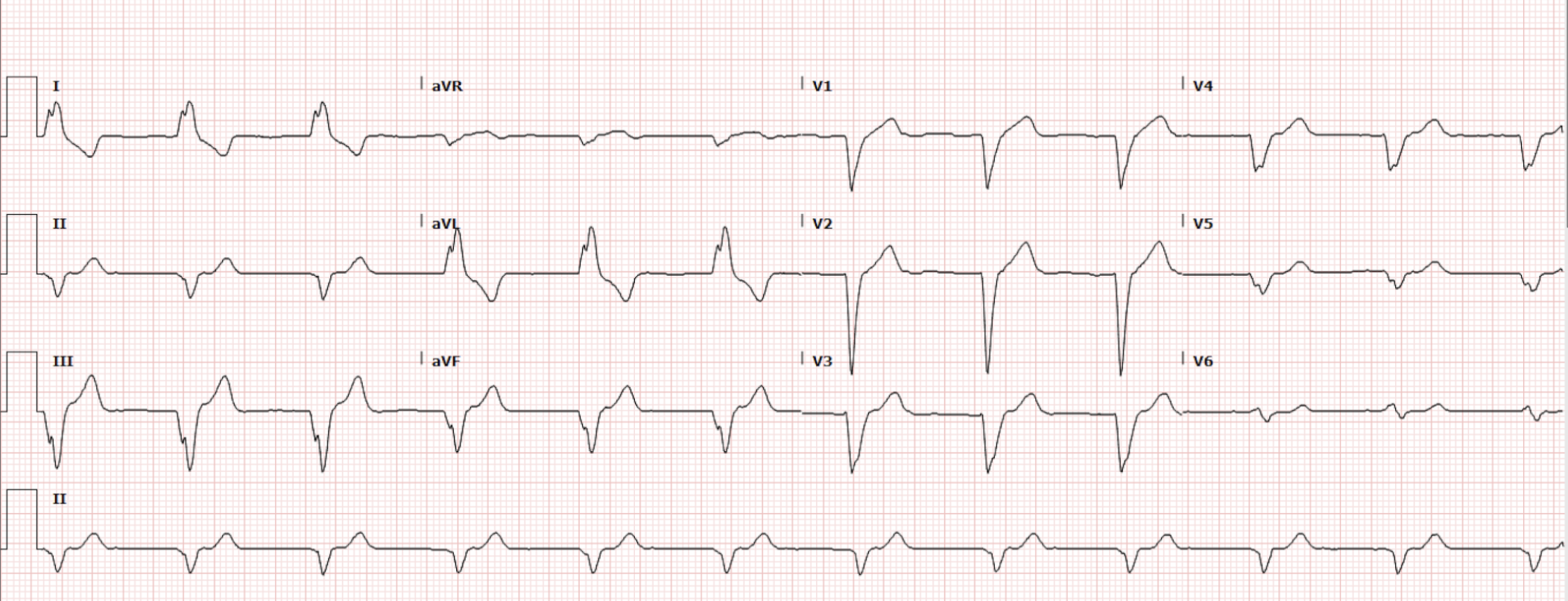
The patient had an EKG done in triage, which is shown below (Figure 1).
Interpretation: Rate: 68 bpm; Rhythm: regular; Axis: Left Axis Deviation (I: pos., II: neg., aVF: neg) Intervals: PR: n/a; QRS: 166 (prolonged); QT: 462; P-Waves: absent?; QRS Complex: prolonged; ST Segment/T-waves: no ST elevation; left bundle branch block morphology.
Taking a closer look by increasing the gain and applying an increased amplitude (Figure 2)…
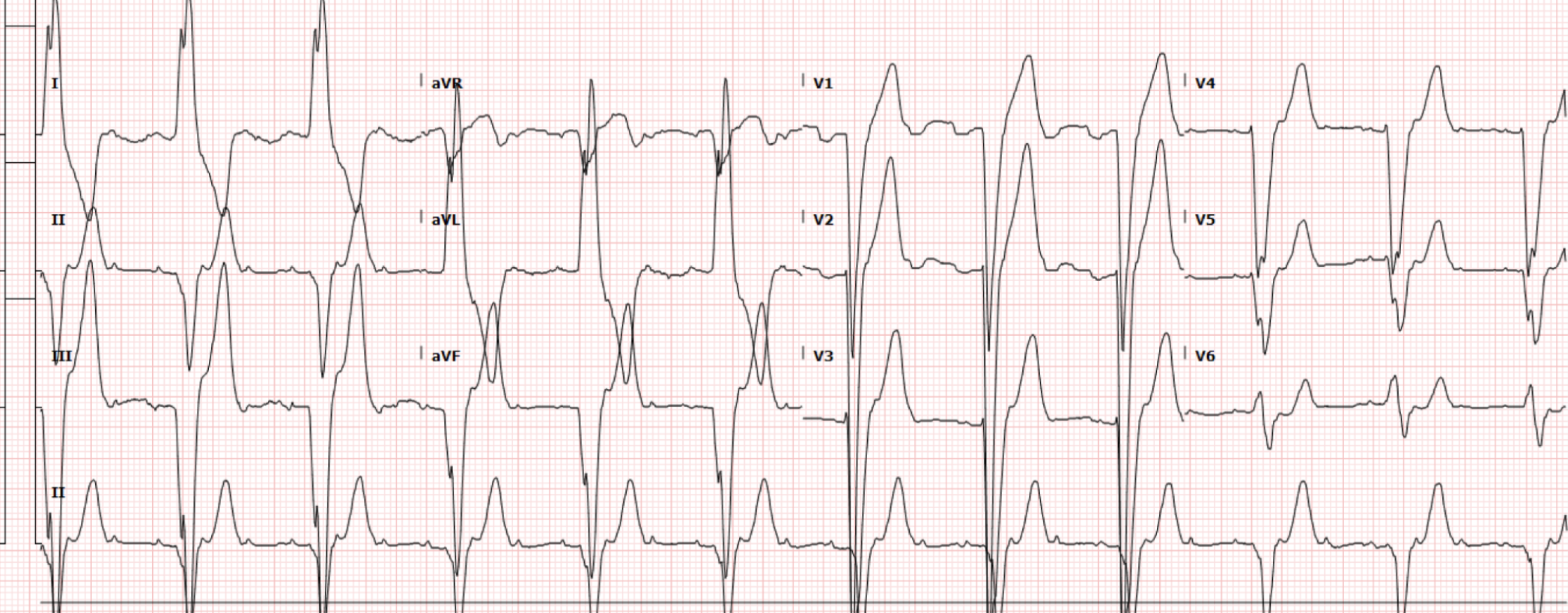
Figure 2. Index EKG with augmented amplitude
…we can now see unique appearing P waves consistent with 3:1 atrial tachycardia, which was confirmed by EP after their review of the EKG.
While in the ED, the patient was noted to have an elevated troponin that was down trending (245 to 196) and a BNP of 500, with a plan for admission initially to an inpatient telemetry unit. However, the patient later had a run of what appeared to be ventricular tachycardia on telemetry monitoring in the ED and a repeat EKG was obtained (Figure 3).
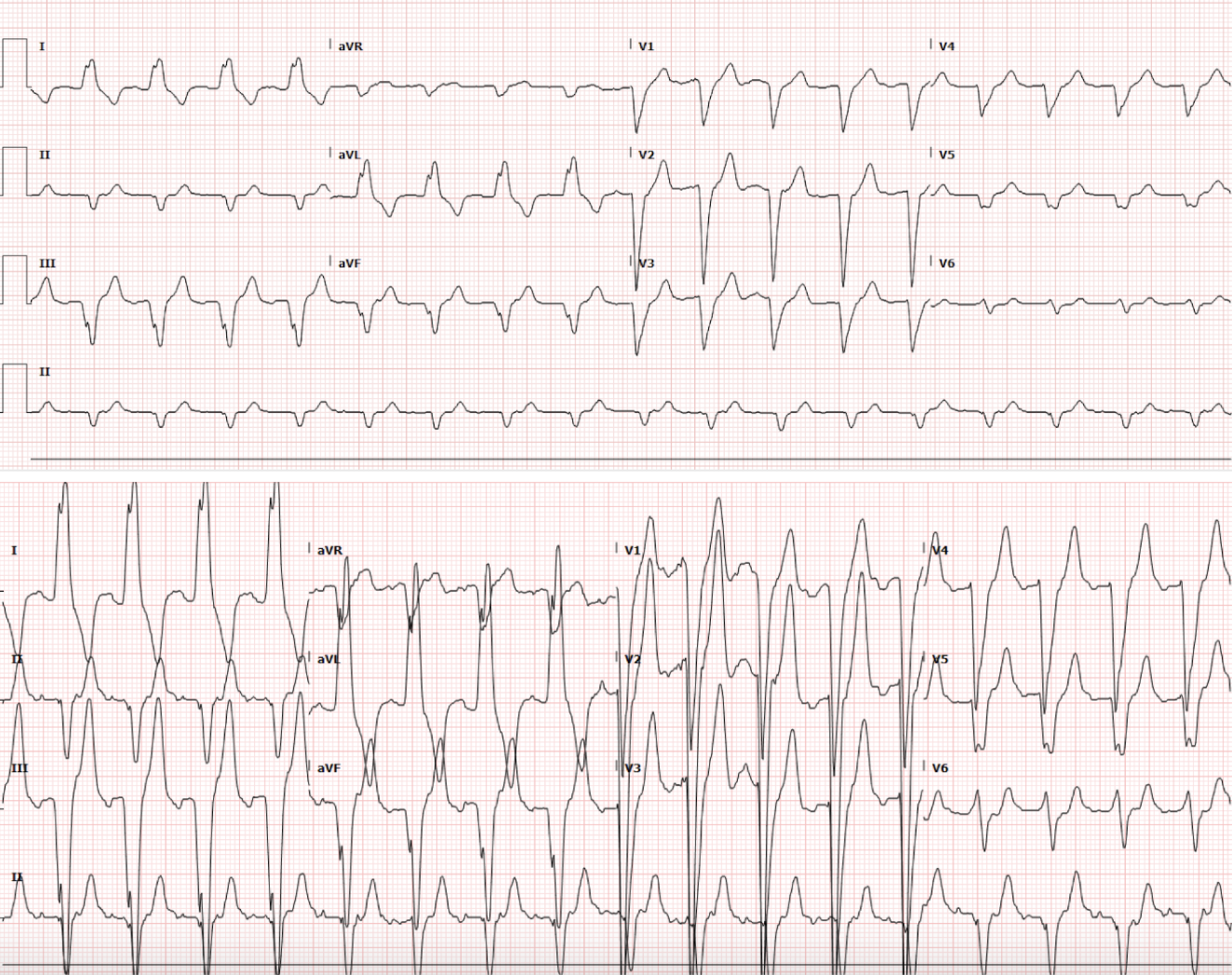
Figure 3. Repeat EKG triggered by asymptomatic tachydysrhythmia
Interpretation: Rate: 104 bpm; Rhythm: regular; Axis: Left Axis Deviation (I: pos., II: neg., aVF: neg) Intervals: PR: 164; QRS: 165 (prolonged); QT: 433; P-Waves: 2:1; QRS Complex: wide; ST Segment/T-waves: no ST elevations, Left bundle branch block
The repeat EKG was similar to the initial EKG, except now with a 2:1 block. The patient was again seen by EP at that time, and what initially appeared to be ventricular tachycardia on the monitor was believed to be likely atrial tachycardia with aberrancy that resolved spontaneously without intervention. Given the resolution of symptoms, a plan was made for outpatient follow-up with EP for ablation, and the patient was to be discharged at the recommendation of cardiology and EP.
However, prior to discharge, the patient’s heart rate spontaneously increased to the 200s, she became dizzy, and was unable to stand on her own. At this time, yet another EKG was obtained (Figure 4).
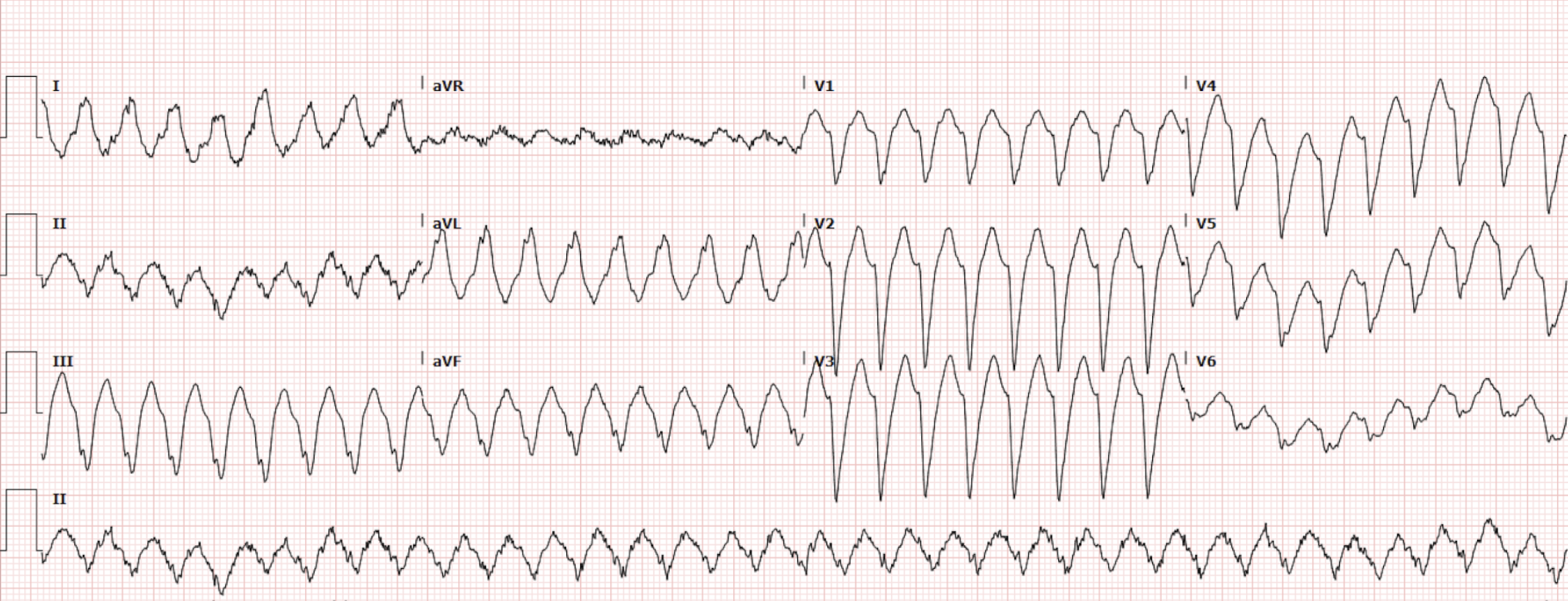
Figure 4. Repeat EKG triggered by symptomatic tachydysrhythmia
Interpretation: Rate: 206 bpm; Rhythm: regular; Axis: undeterrable, Intervals: PR: n/a; QRS: 142 (prolonged); QT: 318, P-Waves: absent; QRS Complex: wide; ST Segment/T-waves: Left bundle branch block morphology
The EKG at this time captured the atrial tachycardia with aberrancy and the patient was given 10mg Metoprolol IV, at the recommendation of EP. Her HR improved to 102, and she was ultimately admitted to the cardiac IMCU for further management.
Discussion
Atrial tachycardia is a type of supraventricular tachycardia that originates from an ectopic focus in the atria rather than in the SA node. It usually has a rate between 100-250 BPM. On EKG, the QRS is narrow due to normal conduction through the His-Purkinje system. Most notable is an abnormal P-wave morphology, abnormal axis, and an isoelectric baseline (which helps differentiate from Atrial Flutter). The rhythm may be unifocal, with a consistent, unique P-wave shape, or multifocal, as in multifocal atrial tachycardia, where there are at least three different P-wave morphologies and an irregular rhythm. It usually results from enhanced automaticity, triggered activity, or micro-reentry, and it is often associated with conditions such as structural heart disease, hypoxia, pulmonary disease, or digoxin toxicity.
Treatment of supraventricular atrial tachycardia usually involves rate control (i.e. beta blockers/calcium channel blockers), rhythm control, or synchronized cardioversion if hemodynamically unstable. Some atrial tachycardias are responsive to adenosine, such as those from triggered activity or microreentry involving the sinus node. Multifocal atrial tachycardia requires identifying the underlying cause. Ablation is usually a definitive treatment for both unifocal and multifocal atrial tachycardia.
In contrast, wide complex atrial tachycardia with aberrancy refers to the same underlying atrial rhythm, but with abnormal conduction through the ventricles, resulting in a widened QRS complex greater than 120ms. The QRS widens due to a bundle branch block or rate-related conduction delay, causing the ventricles to depolarize outside the normal conduction pathways. Although the rhythm still originates in the atria and may retain features such as preceding P waves, these can be more difficult to identify on ECG because of the widened QRS complexes. Clinically, this distinction is important because wide complex atrial tachycardia with aberrancy can closely mimic ventricular tachycardia, as with our case above. When distinguishing between ventricular tachycardia and atrial tachycardia with aberrancy on EKG, VT has identifiable capture beats or fusion beats (see HOTM 12.19.25 for review) vs. atrial tachycardia with aberrancy maintains a consistent relationship between P waves and QRS complexes, often with visible P waves preceding each QRS. Although again, identifying such a feature is challenging when the P wave is not always easily identifiable (such as above).
Treatment for atrial tachycardia with aberrancy is similar to supraventricular atrial tachycardia (as long as there is no accessory pathway), i.e. rate and rhythm control and cardioversion if unstable. However, misidentifying ventricular tachycardia or treating AT with an accessory pathway with AV nodal–blocking agents can be devastating. Hence, it is important to err on the side of caution and treat any regular wide complex tachycardia as ventricular tachycardia when there is doubt, unless after careful review and discussion with EP.
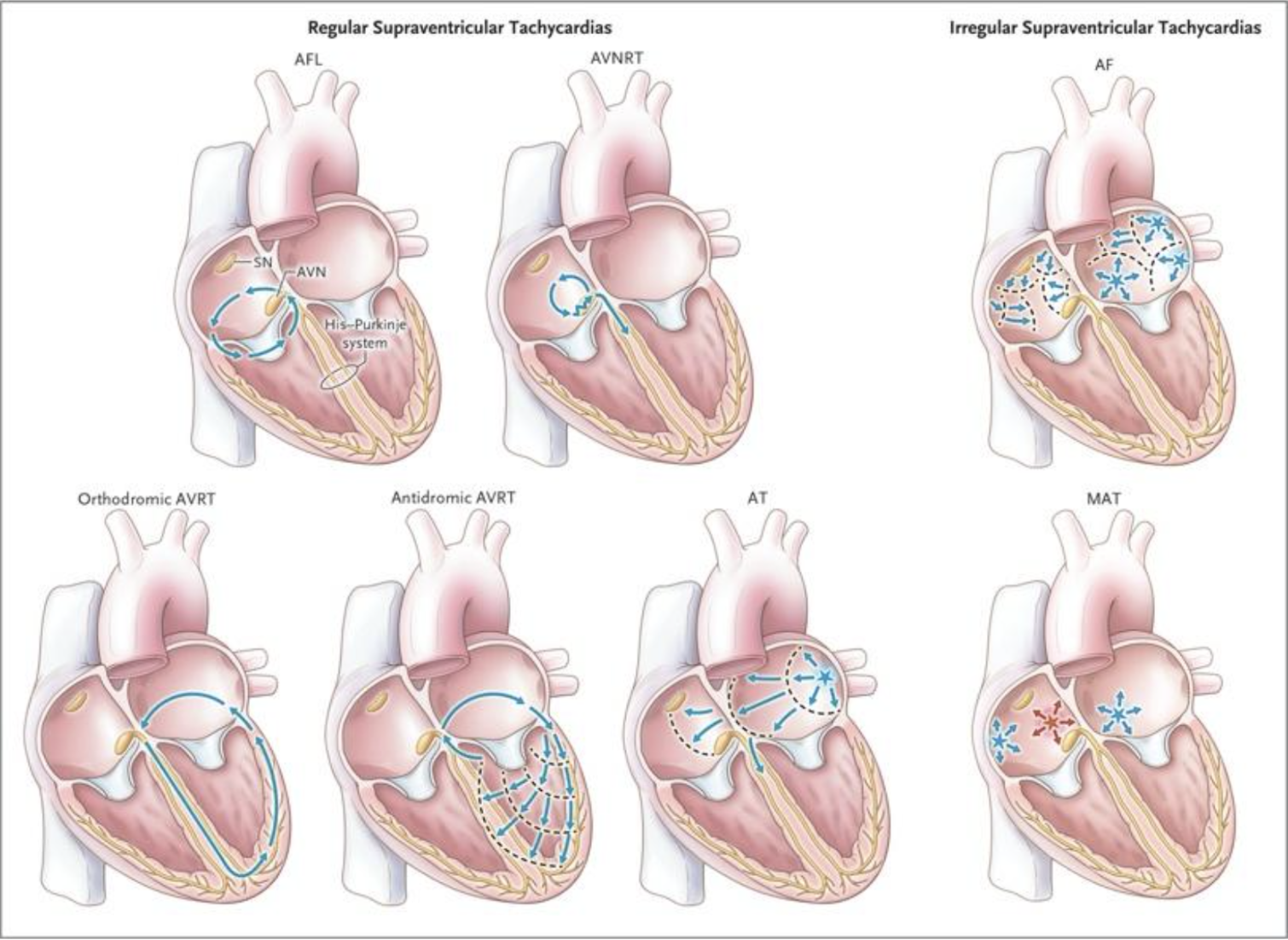
Figure 5. Mechanisms of Supraventricular Tachycardias, According to Regularity of Rhythm (Image from “Guideline for the Management of Adult Patients With Supraventricular Tachycardia”).
Conclusion
Given the patient's two prior EKG and close discussion with EP throughout the course of her case with the suspected diagnosis of atrial tachycardia already made, she was treated as such with beta blockers. It is important to note that this is not the standard approach for a wide complex tachycardia, and the diagnosis of atrial tachycardia with aberrancy should not be made without careful consultation with EP.
The patient was admitted to the IMCU and underwent ablation on 12/2. Following her ablation, she was noted to be in a persistent junctional rhythm for which plans were made for a temporary pacemaker. She was transferred to the CCU and subsequently underwent a permanent pacemaker with a repeat ablation on 12/9 with restoration of a stable rhythm.
Take Home Points
Atrial tachycardia is a type of supraventricular tachycardia that originates in the atria, outside the SA node, with normal conduction through the rest of the heart
Atrial tachycardia with aberrancy also starts in the atria outside the SA node, but has a distinguishable widened QRS complex due to bundle branch block or rate-related conduction delay that causes the QRS to be prolonged
Atrial tachycardia and atrial tachycardia with aberrancy are treated the same way (as long as there is no accessory pathway). However, misidentifying ventricular tachycardia as atrial tachycardia with aberrancy can be detrimental.
A wide complex tachycardia should always be presumed to be ventricular tachycardia and treated accordingly. Beta blockers (or other AV nodal–blocking agents) should not be used empirically in this setting, as they may be ineffective or potentially harmful if the rhythm is ventricular in origin. Treatment as atrial tachycardia with aberrancy should only occur after careful evaluation and explicit guidance from EP.
References
Link MS. Evaluation and Initial Treatment of Supraventricular Tachycardia. New England Journal of Medicine. 2012;367(15):1438-1448. doi:https://doi.org/10.1056/nejmcp1111259
Burns DE. Atrial Tachycardia • LITFL • ECG Library Diagnosis. Life in the Fast Lane • LITFL • Medical Blog. Published August 1, 2018. https://litfl.com/atrial-tachycardia-ecg-library/
Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia. Journal of the American College of Cardiology. 2016;67(13):e27-e115. doi:https://doi.org/10.1016/j.jacc.2015.08.856
Liwanag M, Willoughby C. Atrial Tachycardia. PubMed. Published 2020. https://www.ncbi.nlm.nih.gov/books/NBK542235/
LITFL. Ventricular Tachycardia – Monomorphic VT • LITFL • ECG Library. Life in the Fast Lane • LITFL • Medical Blog. Published March 16, 2019. https://litfl.com/ventricular-tachycardia-monomorphic-ecg-library/
Authored by Emily Bovasso MD and Ari Edelheit MD