
The patient is a 70-year-old female with a past medical history of hypertension, off of medications, who is presenting for concern of chest pain. The pain radiated to both her neck and back, started at 4 AM, and resolved just 10 minutes prior to arrival in the emergency department.
Vital signs:
HR: 125, BP: 180/109, RR: 20, O2: 94% on RA
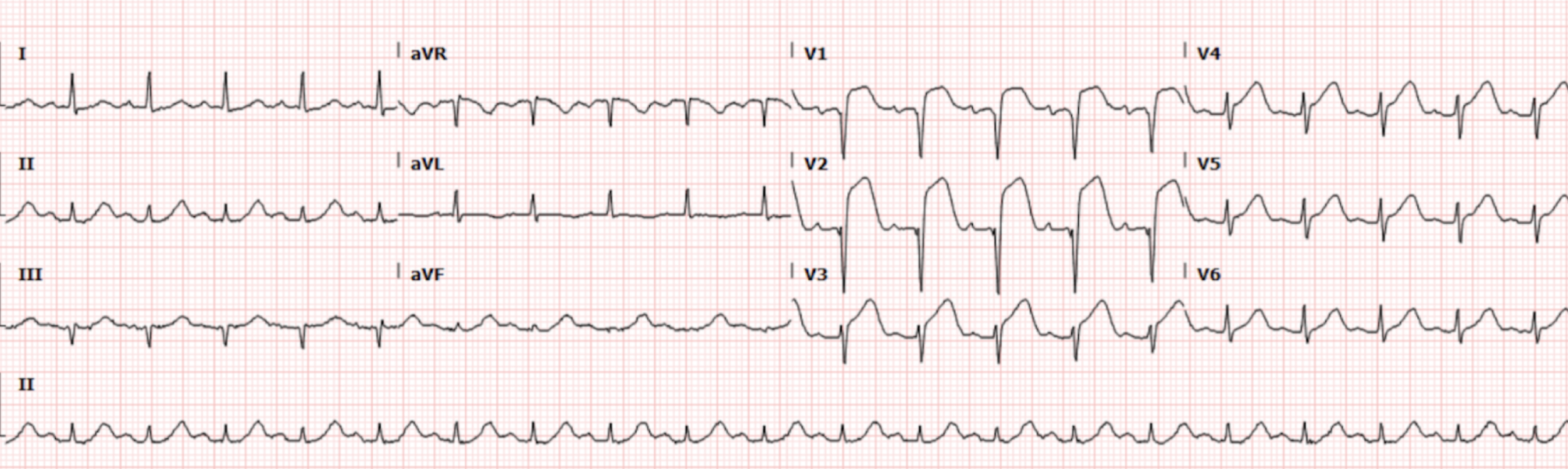
The patient had an EKG (Figure 1) in triage that was immediately brought to the attending for review:
Interpretation: Rate: 125 bpm; Rhythm: regular; Axis: normal (I: pos., II: pos., aVF: pos) Intervals: PR: 172; QRS: 68; QT: 300, normal; P-Waves: normal morphology; QRS Complex: normal width; ST Segment/T-waves: Large ST segment elevation in V1-V4. No obvious reciprocal changes.
Based on the EKG findings above, this patient was noted to be having an acute myocardial infarction. An ED code STEMI was activated immediately on presentation of the patient to the resuscitation bay. Aspirin was administered and bedside echo showed a regional wall motion abnormality of the anterior wall.
Cardiology presented to the bedside and requested further imaging to rule out a dissection, which was performed and was negative, and then took the patient to the cath lab. In the cath lab, they found the patient to have a thrombotic 100% occlusion of the mid-segment of the LAD. Repeat EKG in the CCU 2 days later (Figure 2.), showed evidence of deep Q waves in the anterior leads, as well as some persistent ST segment derangements.
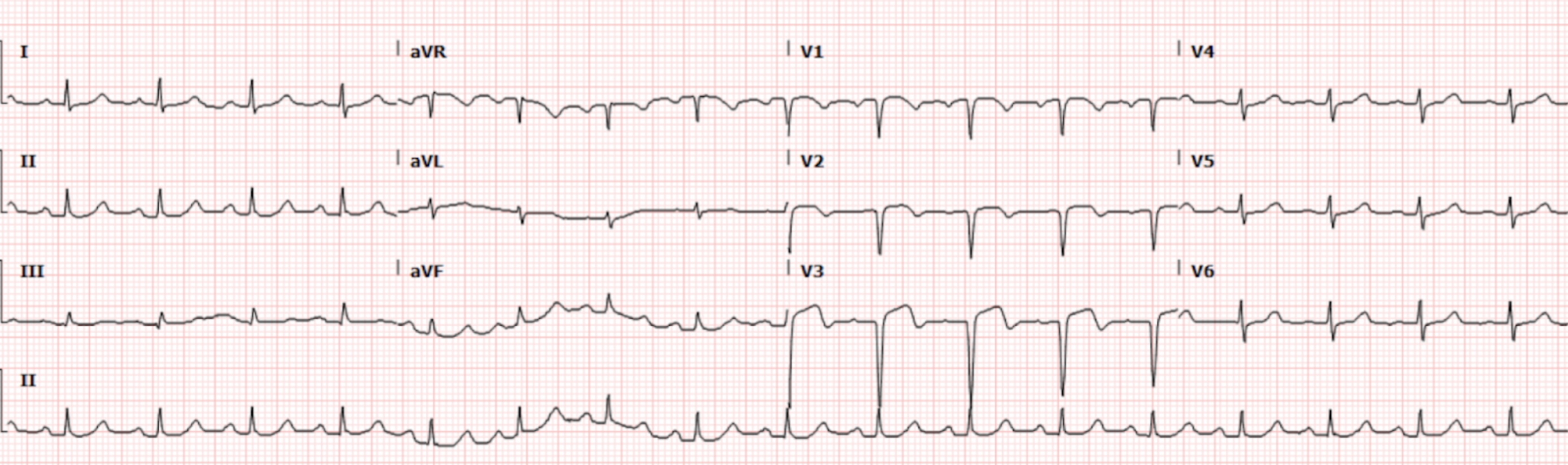
Figure 2. EKG from the CCU 2 days post-presentation
Interpretation: Rate: 105 bpm; Rhythm: regular; Axis: normal (I: pos., II: pos., aVF: pos) Intervals: PR: 146; QRS: 85; QT: 345, normal; P-Waves: normal morphology; QRS Complex: normal width; deep Q waves noted in V1-V3 ST Segment/T-waves: Biphasic ST segment changes in V1-V3
Ultimately, this patient recovered well and is currently following with cardiology as an outpatient.
Discussion
This patient presented with EKG findings concerning anterior STEMI. This EKG exhibits significant ST segment elevation in V1-V4, which is concerning for a significant infarct in the anterior-septal segment. As a review, Table 1 below outlines the region, vessel, and EKG findings for typical STEMI patterns.
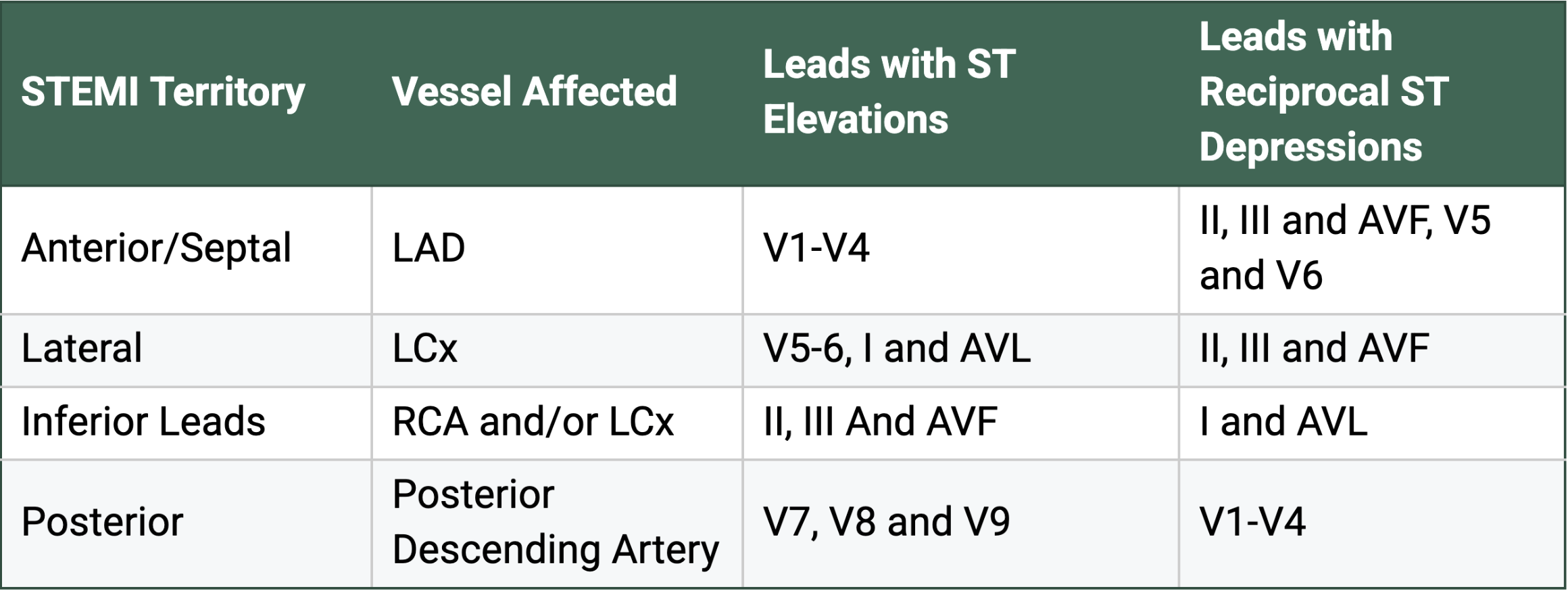
Table 1. Typical STEMI pattern on EKG
The clinicians involved in the case astutely picked up on these EKG findings and immediately activated the code STEMI, which got this patient exactly what they needed: to the cath lab. While the EKG in this case may appear relatively straightforward, there are a few points that are worth a more in depth discussion.
First, we notice that for our case, we do not see any reciprocal changes. This does not rule out an occlusive myocardial infarction. In fact, it is estimated in some studies that only 30% of anterior STEMIs will exhibit reciprocal changes on the EKG.
History and Physical
While this patient presented with a classical chest pain history, it is important to remember that not all patients will present with these symptoms. Particularly, when examining women, they are more likely to have an “atypical presentation” of ischemia. This may include nausea, vomiting, diaphoresis, extreme nervousness, and apprehension. Women are also more likely to exhibit signs of acute heart failure on initial presentation of MI. Additionally, studies have found that women are more likely to experience “prodromal” symptoms for up to a year prior to their MI, including sleep disturbance, fatigue, shortness of breath, and anxiety. For this reason, having a high clinical suspicion for MI and an understanding of anginal equivalents and symptoms in various populations is imperative when working in the emergency department.
Additionally, this patient is noted to be tachycardic. In patients with an acute MI, particularly in the anterior leads, tachycardia is abnormal as we would generally expect bradycardia. This tachycardia can be a sign that a patient has a large myocardial infarction and is more likely to deteriorate into cardiogenic shock.
LAD Occlusion
Our patient was found to have an occlusive thrombus in the Mid-LAD. There are hints on our EKG that can point us to the location of the occlusion if we examine closely, however it is important to note that there is poor correlation between EKG findings and the exact location of blockage found on further testing. For the LAD, there are three distinct areas where occlusions can occur: Proximal, Mid, and Distal. Table 2 below outlines the EKG findings specific to each type of occlusion.
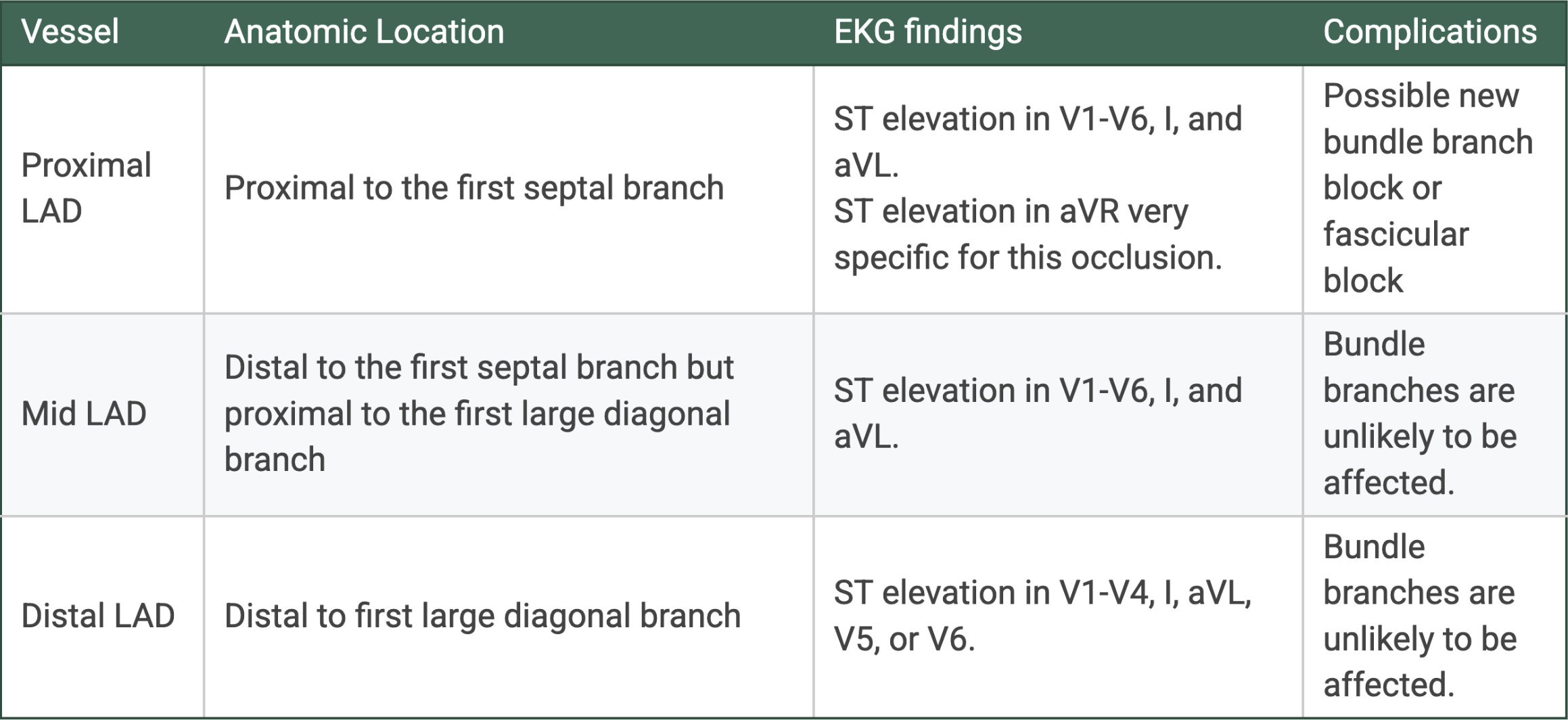
Table 2. EKG findings relative to LAD occlusion location
Our patient did not experience a bundle or fascicular block. This is less suggestive of a proximal LAD occlusion, as we can infer the first large septal branch (which supplies the interventricular septum, and thus the bundle branches) is intact. Our patient exhibited ST elevation in V1-V4, which can be characteristic of both mid and distal LAD occlusion, and ultimately was differentiated via catheterization. Obviously, when it comes to the location of the blockage, the more proximal the blockage is, the more catastrophic damage to the myocardial tissue can be.
Complications
The specific complications following an anterior STEMI are similar to the complications we think about with most types of MIs. However, when compared to inferior infarctions, it has been noted that LAD occlusions have a higher incidence overall of mortality, ventricular arrhythmias, and heart failure. Other complications that may arise include global left ventricular dysfunction secondary to regional wall motion abnormalities and left ventricular mural thrombus formation due to this systolic dysfunction. Our patient was noted to have significant hypokinesis of the anterior wall on echo in the CCU, but was able to maintain an ejection fraction of around 55%.
Take-away Points:
Women can present differently from men when it comes to acute MIs, have a high clinical index of suspicion to obtain an EKG in this population.
Not all STEMIs will have reciprocal changes, while these can be helpful in diagnosis, do not rely on their presence.
LAD occlusions can be catastrophic, and the degree of injury is dependent on the location of the occlusion. While EKG changes can give you some inference as to where the lesion is located, the ultimate test will be catheterization.
In patients presenting with findings concerning for anterior STEMI, be wary of tachycardia and possible ventricular dysfunction leading to symptoms of heart failure. Particularly in women, these may be present at the time of initial presentation.
References:
Sekhon, Navdeep. STEMI. SAEM. 2023. https://www.saem.org/about-saem/academies-interest-groups-affiliates2/cdem/for-students/online-education/m3-curriculum/group-electrocardiogram-%28ecg%29-rhythm-recognition/stemi
Morris F, Brady WJ. ABC of clinical electrocardiography: Acute myocardial infarction-Part I. BMJ. 2002 Apr 6;324(7341):831-4. doi: 10.1136/bmj.324.7341.831. PMID: 11934778; PMCID: PMC1122768.
Schulte KJ, Mayrovitz HN. Myocardial Infarction Signs and Symptoms: Females vs. Males. Cureus. 2023 Apr 13;15(4):e37522. doi: 10.7759/cureus.37522. PMID: 37193476; PMCID: PMC10182740.
Ak R, Doganay F, Onur OO, Akoglu EU. Electrocardiographic clue for a mid-LAD lesion. BMJ Case Rep. 2016 Mar 17;2016:bcr2015213046. doi: 10.1136/bcr-2015-213046. PMID: 26989113; PMCID: PMC4800211.
Burns, Ed. Buttner, R. Anterior Myocardial Infarction. Life in the Fast Lane. October 8, 2024. https://litfl.com/anterior-myocardial-infarction-ecg-library/
Bansal K, Gore M, Afzal M, et al. Anterior Myocardial Infarction. [Updated 2024 Feb 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562234/
Authored by Erica Dolph MD and Ari Edelheit MD