
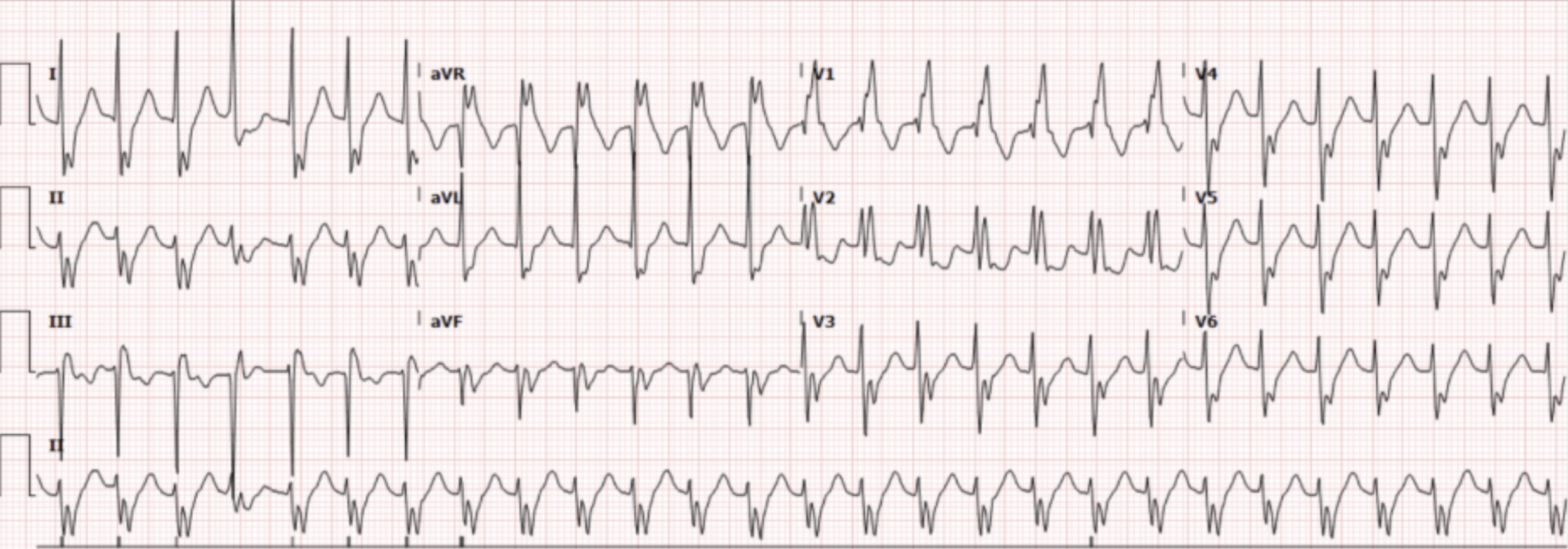
A 74-year-old male with documented 95% stenosis of the LAD in 2021 status post catheterization, HIV well-controlled on Tivicay presents to the ED for intermittent non-exertional, non-pleuritic chest pain that started 2 days ago. The pain is described as non-radiating. He denies any fevers, cough, shortness of breath, lower extremity swelling, abdominal pain, vomiting, diarrhea. He denies prior history of DVT or PE, recent travel, or surgery. Initial vital signs were: BP 163/82, HR 160, RR 20, O2 97% on room air. His EKG (Figure 1) is shown.
Interpretation: Rate: 160 BPM; Rhythm: regular; Axis: left axis deviation (I: pos, aVF: neg); Intervals: PR: 70 (normal), QRS 137 (wide), QTc 416ms (normal), P-waves: not clearly discernable; QRS complex: RSR’ in V1, vV; ST segments/T-waves: ST depressions leads I, aVL, and precordial leads
This patient’s initial rhythm on the cardiac monitor appeared as a regular, narrow complex tachycardia at persistent rates of 150s-160s consistent with SVT. However, after obtaining an EKG, he was found to have a wide complex tachycardia with RBBB morphology. Notably, this was seen on prior EKGs. ]
Modified Valsalva was initially attempted, after which he remained in the above rhythm. He received IV adenosine 6mg followed by 12mg. He initially converted to sinus rhythm with a heart rate in the 80s, however minutes later reverted to SVT. He was given IV metoprolol 5mg which again transiently converted the patient’s rhythm, however, again he reverted to SVT minutes later. Electrical cardioversion was discussed but ultimately it was decided that, given his pattern of converting and reverting suggest aberrancy, and this would likely not be effective.
Cardiology was consulted and they recommended giving another dose of IV metoprolol 5mg and furosemide 20mg IV, which resulted in sustained cardioversion. His initial high sensitivity troponin was elevated to 760, and a repeat was up-trending to 1022. The patient was admitted to CCU and cardiology took the patient for a LHC during which they found the patient had 60% re-stenosis of LAD stent and multivessel disease, for which the patient underwent CABG during his inpatient stay.
Discussion
This case highlighted several important topics.
Ventricular Tachycardia (VT) vs. Supraventricular Tachycardia (SVT) with Aberrancy
Distinguishing regular wide complex tachycardias (WCTs) as VT or SVT with aberrancy is a challenging but important first step in determining appropriate management. Some ECG features that make VT more likely are [1]:
Absence of RBBB or LBBB morphology
QRS complex > 160ms, AV dissociation (P and QRS complexes occur at different rates)
Extreme axis deviation (positive QRS in lead aVF, negative in I, avR)
Positive concordance or negative concordance throughout precordial leads
RSR’ with a taller left rabbit ear
Fusion beats (Figure 2) due to the simultaneous activation of two foci of pacemaker cells – a supraventricular and a ventricular source. This does not occur in pure SVT.
Multiple algorithms that have been validated to help differentiate WCTs, including the Brugada algorithm (Figure 3), Vereckei algorithm, and Basel algorithm (Figure 4). The newer Basel algorithm is arguably the simplest and has a similar specificity and sensitivity to other algorithms. Also, average time to diagnosis has been shown to be significantly shorter using the Basel algorithm (median 38 sec) compared to the Brugada algorithm (median 106 sec) [2]. If there is any uncertainty in the diagnosis of the WCT, the safest option is to treat the patient’s WCT as VT! This will avoid any hemodynamic collapse that could ensue from giving a patient with VT calcium channel or beta-blockers.
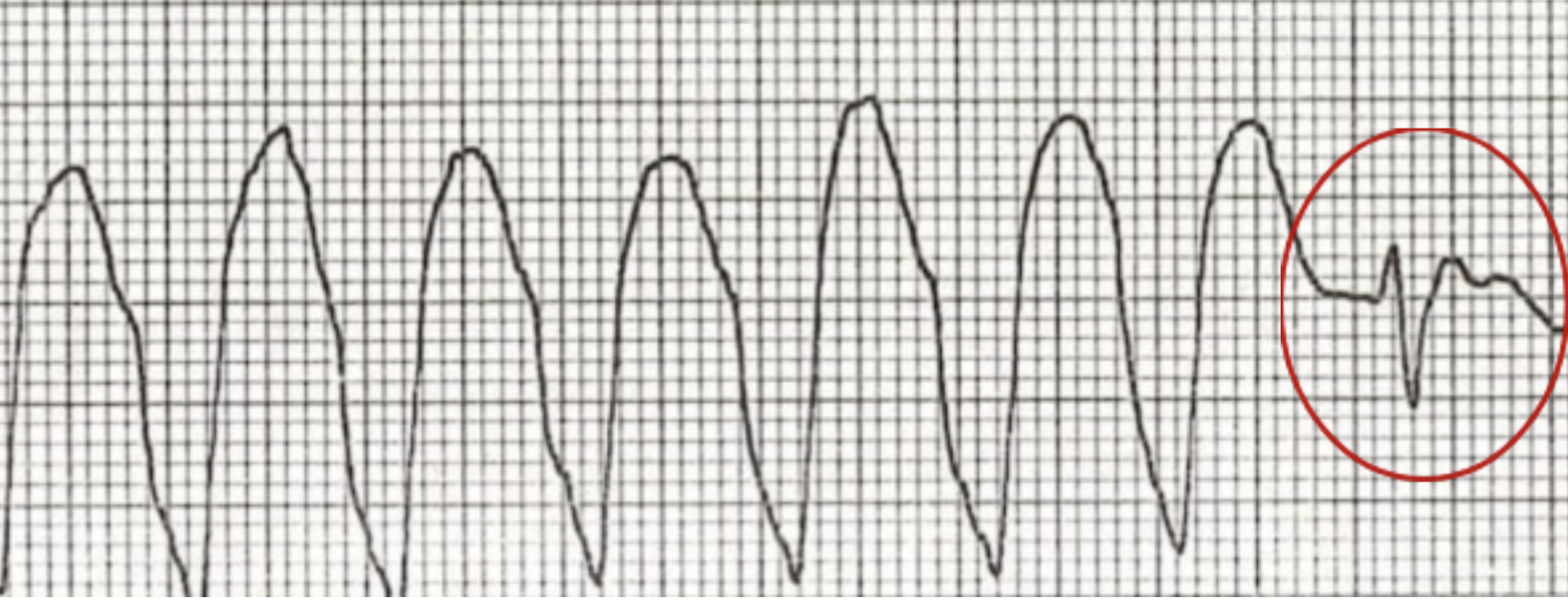
Figure 2. Fusion Beat (Image from: https://litfl.com/fusion-beat-dressler-beat-ecg-library/ )
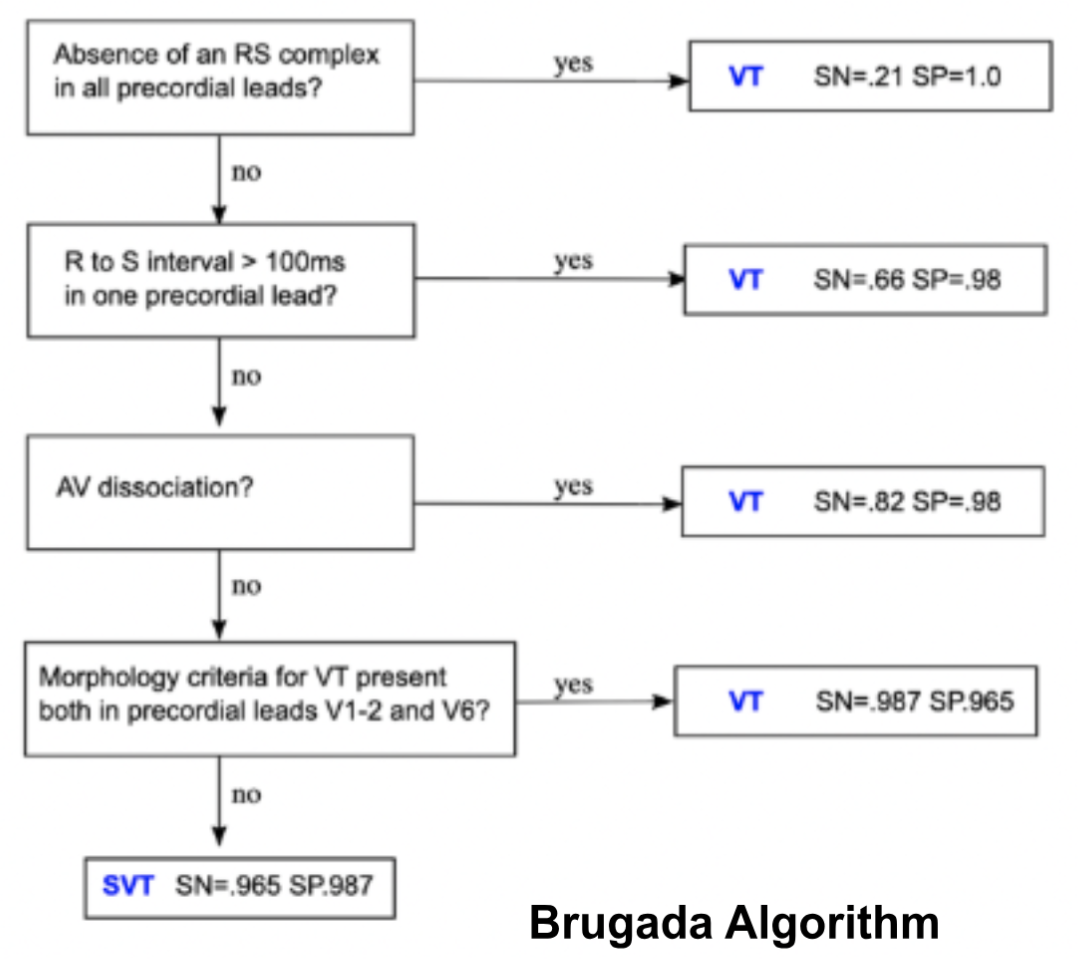
Figure 3. Brugada Algorithm (Image from: https://litfl.com/vt-versus-svt-ecg-library/ )
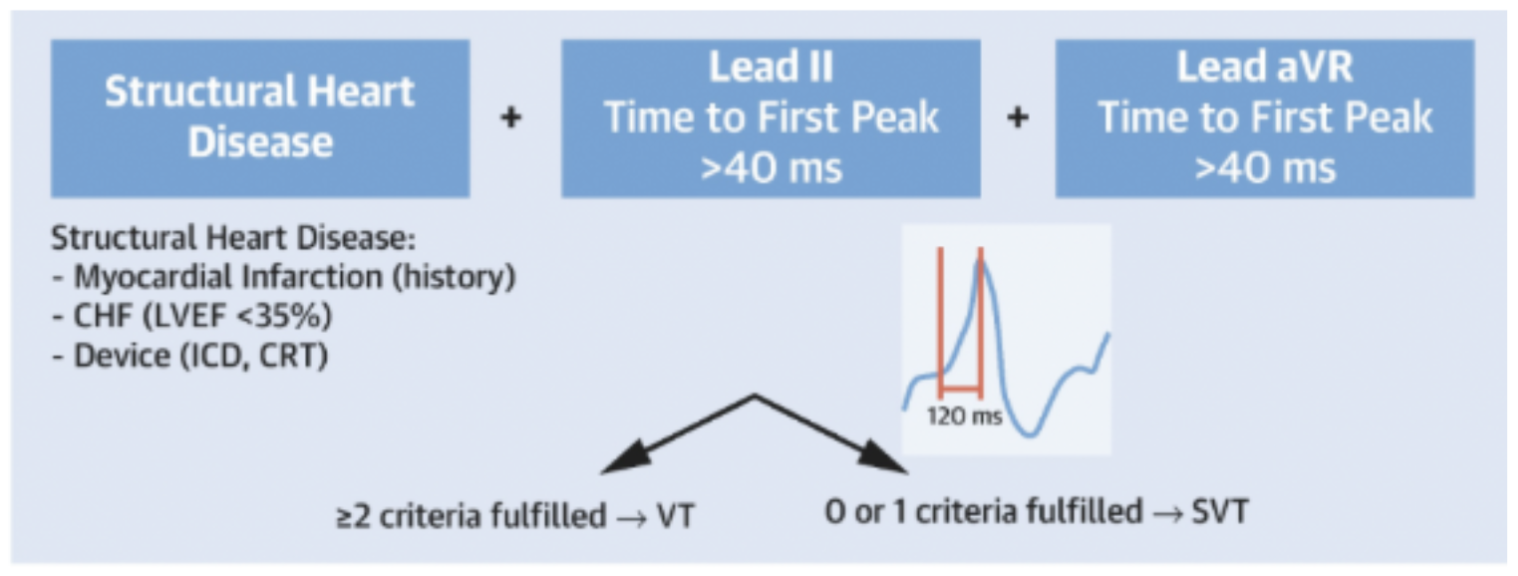
Figure 4. Basel Algorithm (Image from: https://www.jacc.org/doi/10.1016/j.jacep.2022.03.017 )
What Should You Do if the Patient Converts Out of SVT... And Then Goes Back Into It?
Adenosine has a conversion success rate of up to 98% in hemodynamically stable patients with SVT. If an initial bolus is unsuccessful, a second bolus of adenosine at a higher dose can be given. At that point, if the rhythm persists, cardioversion can be used in stable patients except if having spontaneous termination and reinitiation of SVT, according to the American College of Cardiology practice guidelines [3]. This is because this pattern suggests that there is a re-entry circuit. These aberrant pathways are often triggered by atrial or ventricular premature complexes. While a single shock may interrupt the re-entry circuit and cause acute termination, it does not address the underlying cause of the arrhythmia, which may be the premature complexes that are triggering re-initiation.
The next steps for these patients should be pharmacological therapy with IV diltiazem or verapamil, which are longer acting than adenosine and suppress the underlying substrates [4]. It is imperative to first ensure that your patient is not in VT prior to giving either of these drugs and be aware of the risk for hypotension from these agents in all-comers, which can be lessened with slow administration over 20 minutes. While beta blockers are also safe, there is limited evidence on their efficacy in terminating SVT in these cases. Ultimately, patients who are spontaneously going in and out of SVT need a cardiology consult for an EP study and ablation.
To Trop or Not to Trop? A Note on SVT and MI
Troponin elevation is seen in up to 50% of patients with SVT and, in a vast majority of otherwise healthy patients, this reflects a Type II MI due to supply-demand mismatch precipitated by the tachycardia [5]. Therefore, in young patients without CAD risk factors, troponin testing may lead to unnecessary resource utilization. In some cases, however, SVT precipitates MI due to tachycardia-induced shear stress causing plaque rupture [6]. In patients who are high risk (ongoing chest pain, marked ischemic ECG abnormalities such as deep or localized depressions or T-wave inversions, hemodynamic instability, known CAD, or significant comorbidities), consider the possibility of MI precipitating SVT (for example, the patient in our case). Older studies have shown that SVT during the first 4 days of MI is associated with larger infarctions and higher in-hospital mortality than patients with acute MI without SVT [7]. Figure 5 illustrates a proposed framework for sending troponins on patients with SVT in the ED [5].
Figure 5.
Image from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12678887/#sec8
Take Home Points
When in doubt, treat as VT. However, many clues and algorithms exist that can help differentiate WCTs on closer EKG analysis.
If the patient is spontaneously converting out of SVT and reverting despite adenosine, cardioversion is NOT recommended. IV calcium channel blockers, beta blockers, or antiarrhythmics can be used for electrical substrate control and consult cardiology for EP study and likely ablation.
When considering ordering a troponin, clinical context is important. Consider the possibility of ACS as a trigger for SVT in patients who are high risk.
References
Burns, E., Buttner, R., & Buttner, E. B. and R. (2024, October 8). VT versus SVT. Life in the Fast Lane • LITFL. https://litfl.com/vt-versus-svt-ecg-library/
Moccetti, F., Yadava, M., Latifi, Y., Strebel, I., Pavlovic, N., Knecht, S., Asatryan, B., Schaer, B., Kühne, M., Henrikson, C. A., Stephan, F., Osswald, S., Sticherling, C., & Reichlin, T. (2022). Simplified Integrated Clinical and electrocardiographic algorithm for differentiation of wide QRS complex tachycardia. JACC. Clinical Electrophysiology, 8(7), 831–839. https://doi.org/10.1016/j.jacep.2022.03.017
Page, R. L., Joglar, J. A., Caldwell, M. A., Calkins, H., Conti, J. B., Deal, B. J., Estes, N. M., Field, M. E., Goldberger, Z. D., Hammill, S. C., Indik, J. H., Lindsay, B. D., Olshansky, B., Russo, A. M., Shen, W., Tracy, C. M., & Al-Khatib, S. M. (2015). 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients with Supraventricular Tachycardia. Journal of the American College of Cardiology, 67(13), e27–e115. https://doi.org/10.1016/j.jacc.2015.08.856
Wigginton, J. G., Agarwal, S., Bartos, J. A., Coute, R. A., Drennan, I. R., Haamid, A., Kudenchuk, P. J., Link, M. S., Panchal, A. R., Pelter, M. M., Del Rios, M., Rodriguez, A. J., Perman, S. M., Sanko, S., Kotini-Shah, P., & Kurz, M. C. (2025). Part 9: Adult Advanced Life Support: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 152(16_suppl_2), S538–S577. https://doi.org/10.1161/cir.0000000000001376
Özlek, B., Tanık, V. O., & Barutçu, S. (2025). Troponin elevation in supraventricular tachycardia: A narrative review. World Journal of Cardiology, 17(11), 113411. https://doi.org/10.4330/wjc.v17.i11.113411
Subramanian, A., & Lysander, A. (2012). Unusual presentation of acute myocardial infarction. Indian Pacing and Electrophysiology Journal, 12(5), 233. https://doi.org/10.1016/s0972-6292(16)30547-2
Tomás, J. G., Moreno, A. M., Alberola, A. G., Polo, M. B., Aranaga, F. M., & Fernández, S. R. (1999). Incidencia, características clínicas y significación pronóstica de las taquiarritmias supraventriculares en el infarto agudo de miocardio. Revista Española De Cardiología, 52(9), 647–655. https://doi.org/10.1016/s0300-8932(99)74984-5
Authored by Veda Ravishankar MD and Ari Edelheit MD