
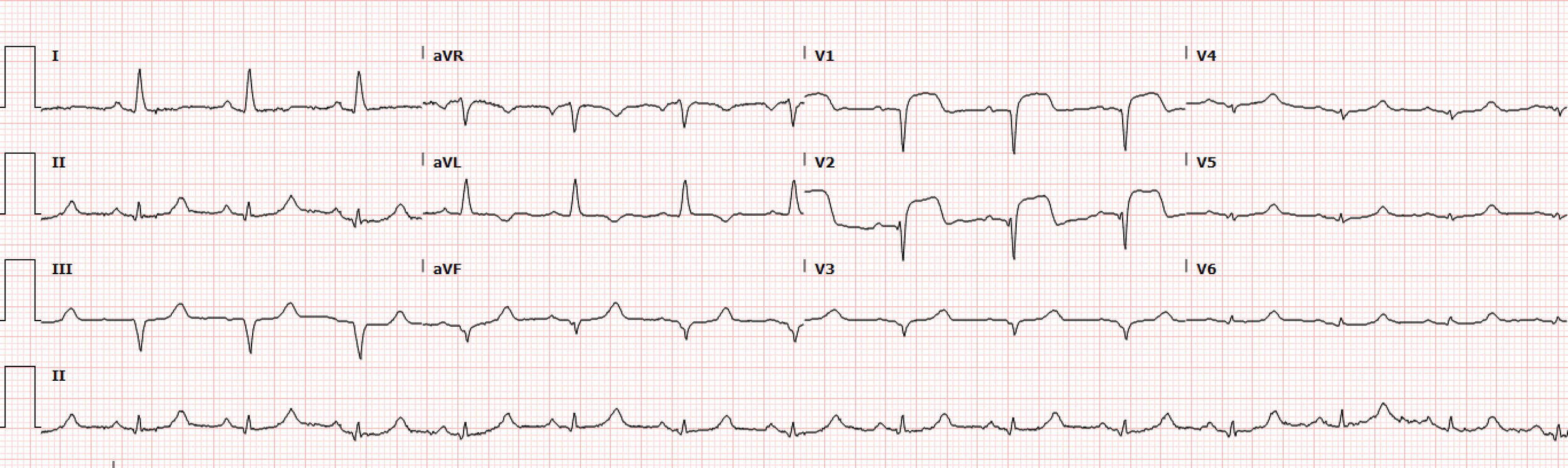
A 57-year-old female with hypertension and diabetes presented with chest pain for the past 3 days with acute change in severity 1-2 hours prior to arrival. A triage EKG was obtained (Figure 1) and the patient was brought to the resuscitation bay.
A repeat EKG was ordered (Figure 2) which demonstrates a unique pathologic finding, as well a contiguous elevation with reciprocal changes, which confirms the suspected diagnosis.
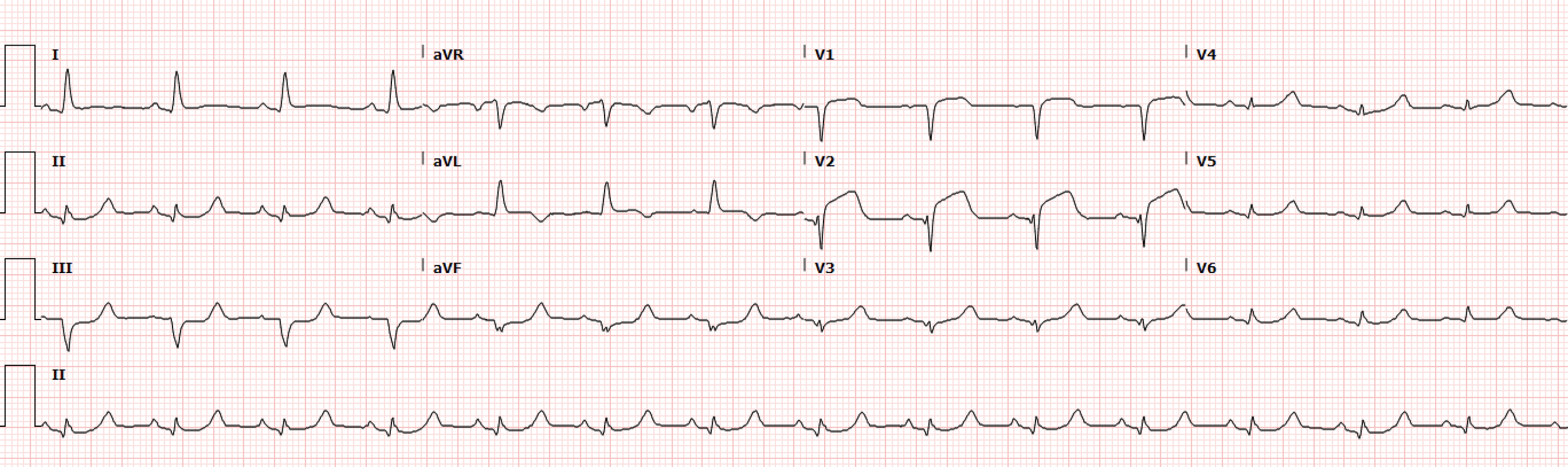
Figure 2. Repeat EKG
Interpretation: Rate: 90 bpm; Rhythm: normal sinus; Axis: normal axis (I: pos., II: pos., aVF: neg); Intervals: PR: 120, normal; QRS: 80, normal; QT: 360, normal; P-Waves: normal morphology; QRS Complex: normal, low precordial voltage, poor R wave progression; ST Segment/T-waves: ST elevations in leads V1-V2, flattened slight ST depressions in V5-V6, reciprocal ST depressions in II, III, aVF
Point-of-care ultrasound demonstrated a large regional wall motion abnormality in the LAD distribution and a STEMI activation was called. The patient was taken to the cath lab with Cardiology which demonstrated a large sized, mid segment 100% occlusion (TIMI 0) and distal LAD (after intervention) with severe diffuse disease. The patient was admitted to the CCU for post-intervention monitoring and was ultimately discharged from the hospital on day 3.
Discussion
The pathologic electrocardiographic findings demonstrated in this EKG (Figure 2) are known as the Precordial Swirl Sign. This finding was described in the Journal of Electrocardiology in 2025 by Goss et al. which found that among 265 included who had OMI, 23 patients were identified by the precordial swirl sign, 19 (83%) of which had LAD culprit lesions, and 16 (70%) of which were missed by traditional STEMI criteria [1]. This finding is due to a proximal LAD occlusion (usually before the first segmental branch) resulting in transmural ischemia of the apex (STD V5-V6) and anteroseptal wall (STD V1-V2).
Mimics of the precordial swirl sign include:
Left Ventricular Hypertrophy
Left Bundle Branch Block
Ventricularly Paced Rhythms
Subendocardial Ischemia
So how do we recognize and differentiate the precordial swirl from its mimics?
The precordial swirl sign first should be suspected when we see ST elevations in V1 and V2. In the above mimics, ST elevation is seen in V2 and V3 but is less frequently seen in V1. As such, when there is significant ST elevation in V1, OMI should be considered [2-3].
Moving on the V5-V6, the morphology of the ST depression itself is often the key to diagnosing the precordial swirl and resultant LAD occlusive OMI. The ST depressions often demonstrate a flatter appearance than in the mimics and should again prompt you to consider OMI. When these two electrocardiographic findings are considered together with concerning clinical symptoms, the diagnosis is OMI until proven otherwise. Looking at the EKG in our case (Figure 3), we see both the ST segment elevation with T-wave inversion (T waves in V1 are negative) and abnormally flattened and depressed ST segments in V6 [2-3].
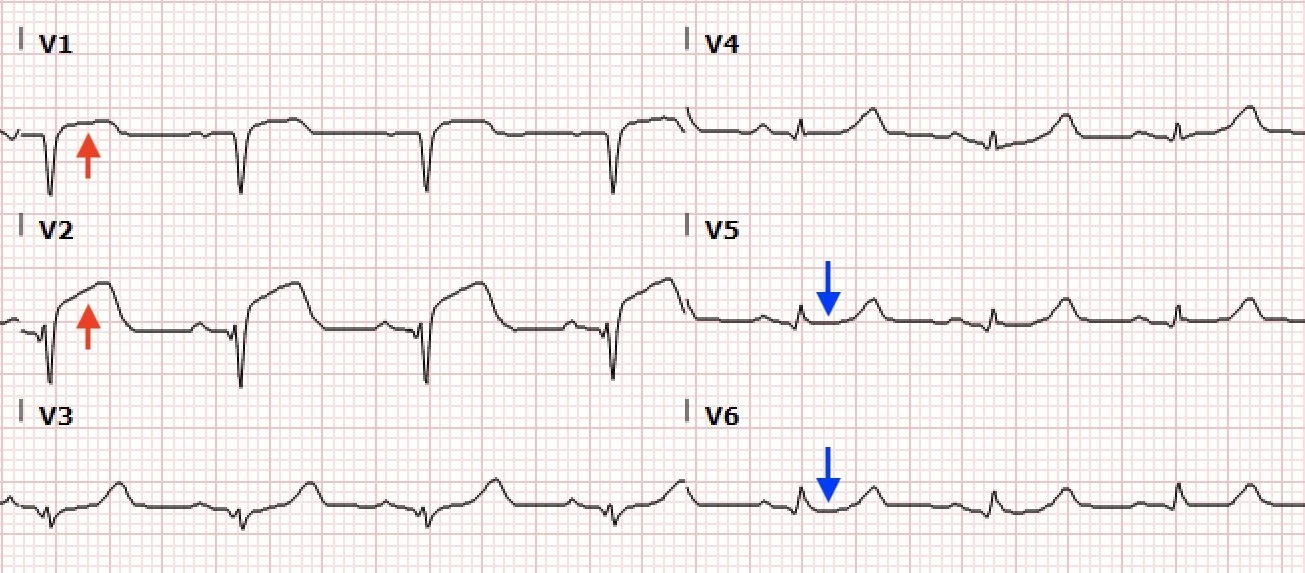
Figure 3. Precordial Swirl
Take Home Points
Any ST Depression in the precordial leads is abnormal
Suspect precordial swirl when you have abnormal or atypical ST elevation in V1 and flat atypical ST depression in lead V6, especially when LVH and other potential mimics are absent
As demonstrated in the study on precordial swirl, traditional STEMI criteria MISSES acute occlusive myocardial infarctions! If there are concerning findings on the EKG, get cardiology on board early and make your case for OMI over STEMI
References
Goss L, Meyers HP, Friedman B, Bracey A, Smith SW. Precordial swirl sign: A new ECG pattern of left anterior descending artery occlusion myocardial infarction. J Electrocardiol. 2025;91:153931. doi:10.1016/j.jelectrocard.2025.153931
Smith S. Precordial Swirl - 20 cases of swirl or look-alikes. Dr. Smith’s ECG Blog. June 27, 2025. Accessed May 17, 2026. https://drsmithsecgblog.com/precordial-swirl-20-cases-of-swirl-or/.
ECG blog #380 - what is “swirl”? ECG Interpretation. Accessed May 17, 2026. https://ecg-interpretation.blogspot.com/2023/05/ecg-380-what-is-swirl-metodo.html.
Authored by Michael Hohl MD and Ari Edelheit MD