
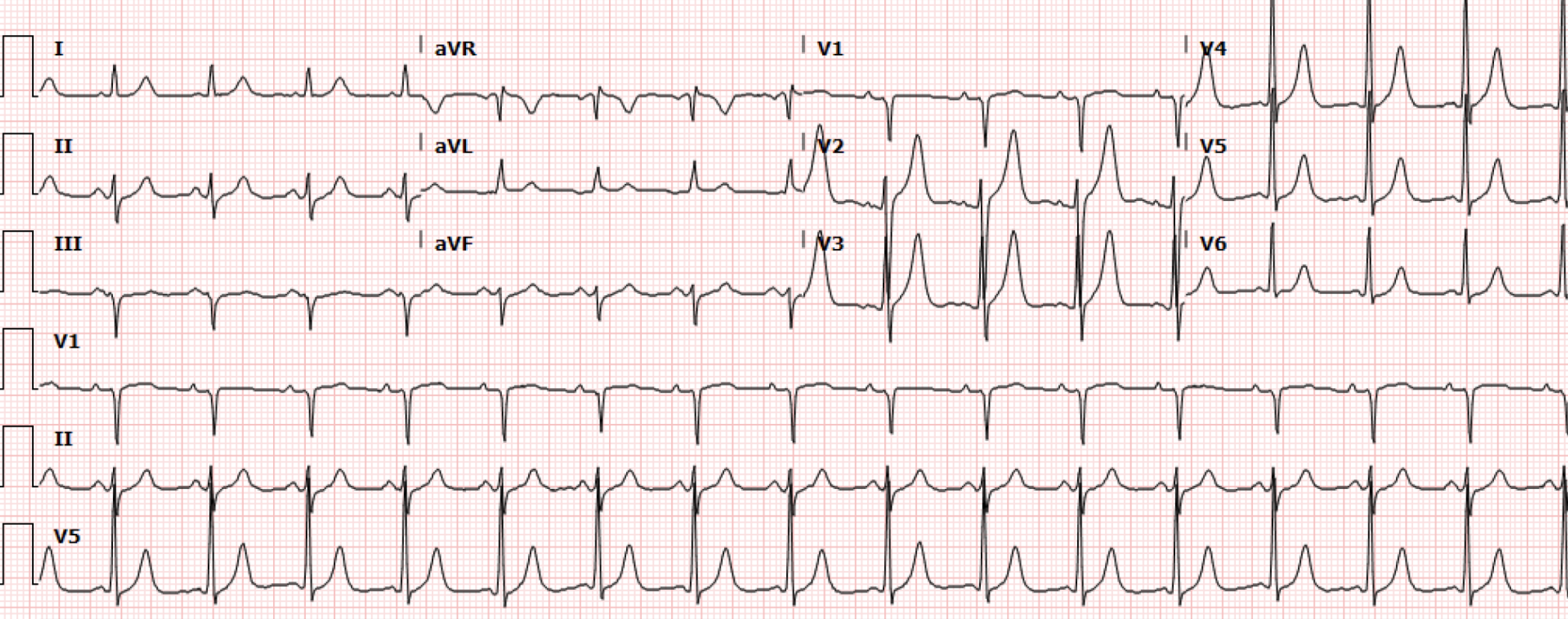
A 61-year-old male with a history of asthma and opioid use disorder presented to the emergency department with acute worsening of shortness of breath, chest pain and cough associated with blood tinged sputum for two weeks. The patient also endorsed chronic heroin use; last use was 1 bag of heroin around 24 hours prior to presentation. The patient denied use of anticoagulation, prior DVT or PE, travel, recent surgery, or known cancer history. The patient's initial EKG (Figure 1) is shown below (0224).
Interpretation: Rate: 95bpm; Rhythm: sinus rhythm; Axis: left (I: pos., II: biphasic., aVF: neg); Intervals: PR: 117; QRS: 78; QT: 381 ; P-Waves: normal; QRS Complex: normal; ST Segment/T-waves: no ST elevation, symmetric peaked T waves V2-V5
The initial labs were notable for K 4.5, troponin 157, and D-dimer of 8. Bedside echo demonstrated findings of D sign and flat IVC. A CT angiogram of the chest was ordered and on return, the patient was found to have a heart rate of 170s on telemetry. A repeat EKG (Figure 2) was ordered stat (0545):
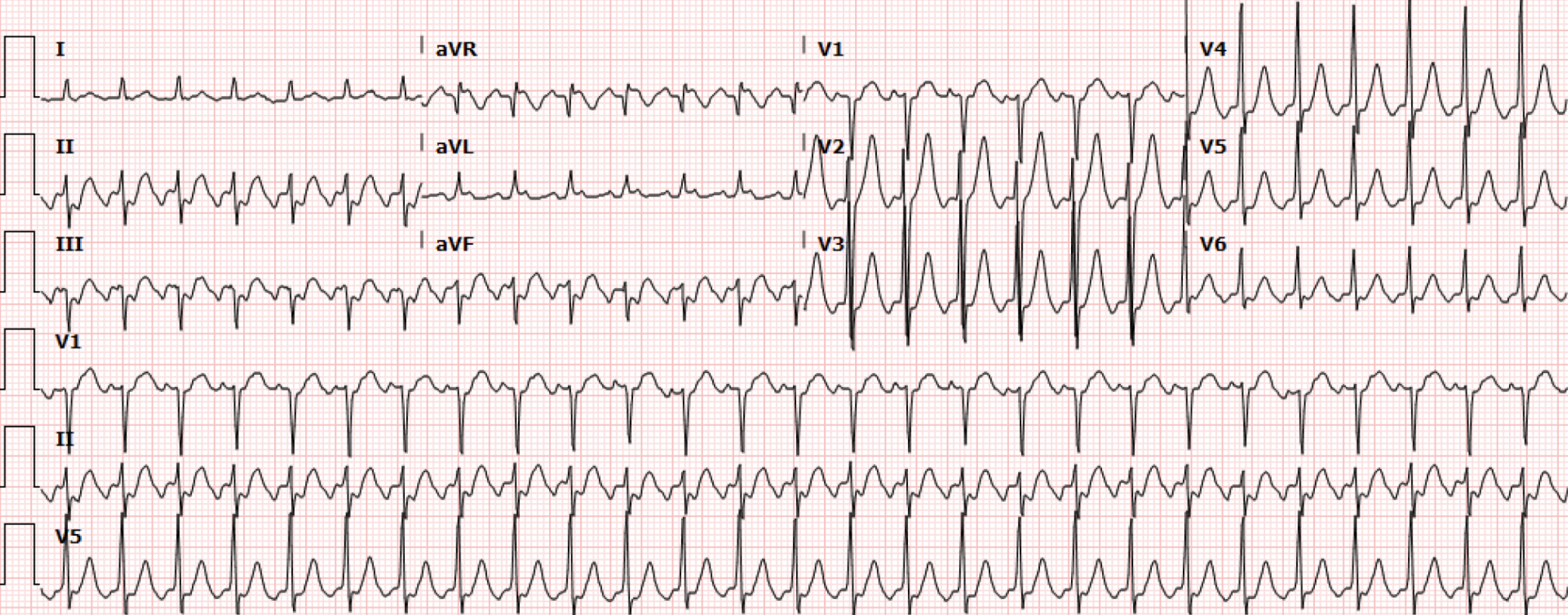
Figure 2. Repeat EKG after change in HR on monitor
Interpretation: Rate: 163bpm; Rhythm: atrial; Axis: left (I: pos., aVF: neg); Intervals: PR: N/A; QRS: 74 QT: 326; P-Waves: possibly superimposed with QRS; QRS Complex: narrow complex; ST Segment/T-waves: no ST elevation, symmetric peaked T waves V2-V5
The CTA chest showed a right lung consolidation and evidence of right heart strain and the PERT team was activated. The patient was also treated empirically for community acquired pneumonia. Cardiology was present at the bedside and the rhythm was thought to be an SVT. The patient was initially given 6mg of adenosine with improvement in the HR. However, within 5 minutes, the patient’s HRs returned to the 160s. The patient was subsequently given another 6mg of adenosine and a third EKG (Figure 3) was obtained (0819):
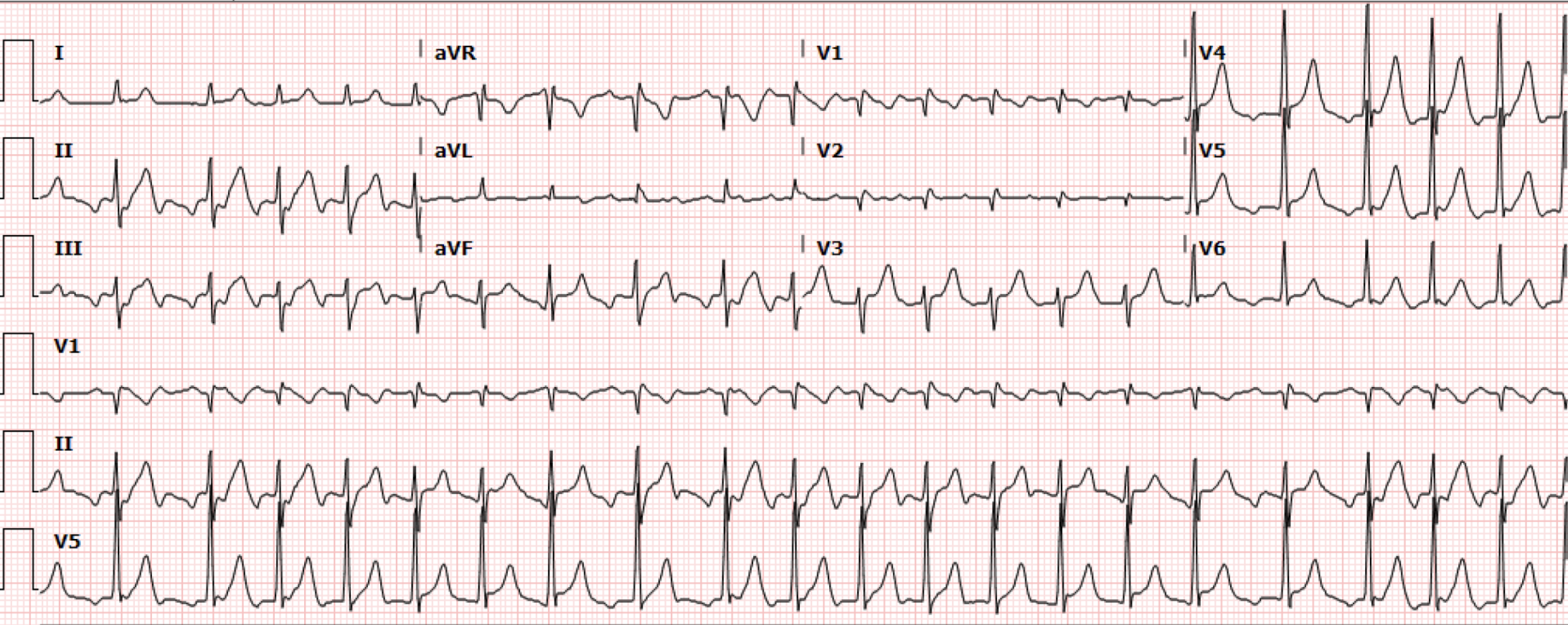
Figure 3. Repeat EKG after adenosine failure
Interpretation: Rate: 126bpm; Rhythm: atrial;Axis: left (I: pos, II: pos, aVF: neg); Intervals: PR: N/A; QRS: 81 QT: 358; P-Waves: sawtooth P waves 2:1 conduction ; QRS Complex: narrow complex; ST Segment/T-waves: no ST elevation or T waves changes
This EKG (Figure 3) demonstrated a slightly lower HR which revealed the underlying rhythm of likely 2:1 atrial flutter. Cardiology recommended 5mg IV metoprolol for three doses and subsequent transition to PO metoprolol. The patient was admitted to the CCU.
During the CCU course, the patient was started on a diltiazem drip to ultimately achieve rate control. Cardiology diagnosed the patient with atrial flutter with the suspected etiology of thought to be secondary to either from fentanyl withdrawal or community acquired pneumonia.
Discussion:
On presentation, the patient was complaining of vague symptoms and the initial EKG showed normal sinus rhythm, as seen in Figure 1. Subsequently, the patient was noted to be in a rapid atrial rhythm (Figure 2) which ultimately, after rate control, was determined to be Atrial Flutter with 2:1 Conduction. The differential was broad, including pulmonary embolism, myocardial infarction, substance-induced arrhythmia, and sepsis from community acquired pneumonia.
Atrial flutter is a supraventricular rhythm that is characterized by a fixed, tachycardic atrial rate generally around 300 bpm. This high rate is facilitated by a re-entrant circuit in the atria, most commonly originating in the tricuspid isthmus. The characteristic EKG finding is the “sawtooth” pattern without a clear isoelectric line connecting the P and QRS complexes as we would normally expect. This sawtooth pattern can clearly be seen in Figure 3. Conduction to the ventricles can vary because of their increased refractory period. In atrial flutter, this produces ventricular conduction blocks that are typically 1:1, 2:1, 3:1, or 4:1. The image in Figure 4 depicts what each of these conduction rates look like. This ventricular rate can either be set or variable.
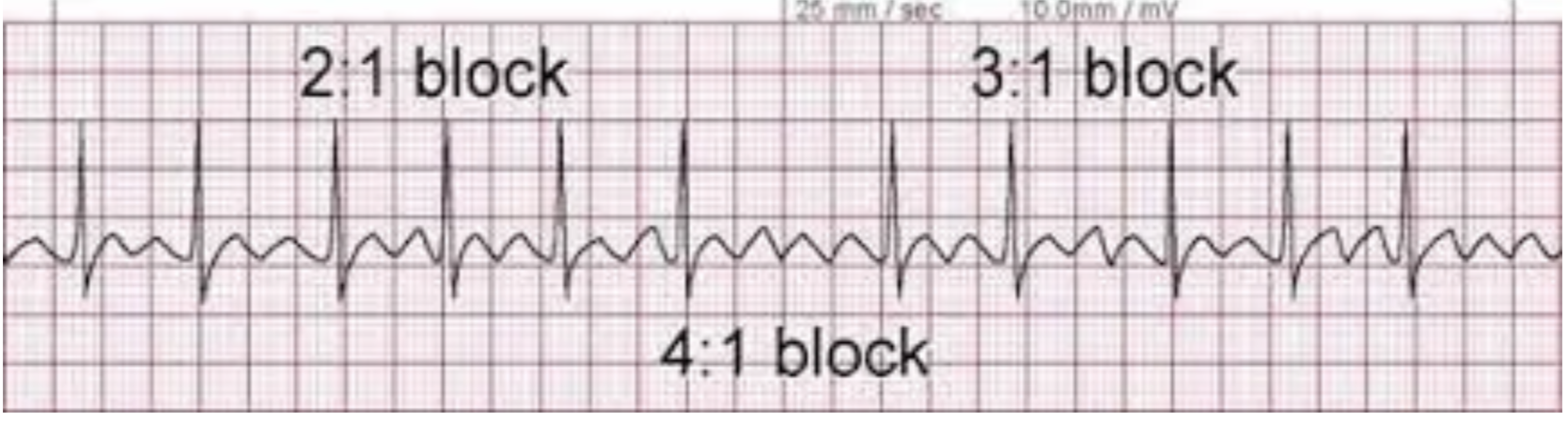
Figure 4. Atrial Flutter with variable conduction (Image from: https://rushem.org/atrial-flutter-av-blocks/)
While atrial flutter is one of the most common types of supraventricular arrhythmias, its causes can vary substantially. It can be seen in patients with underlying pulmonary disease (such as our patient with a history of smoking and a newly diagnosed pneumonia), pulmonary hypertension, heart disease, substance use, presence of other comorbidities such as hypertension, diabetes, and older age. Our patient had many of these risk factors.
The EKG in Figure 2 and 3 is suggestive of Atrial Flutter with a 2:1 block, particularly if you pay close attention to lead II, where you can see that distinct sawtooth pattern. Please see Figure 5 below:
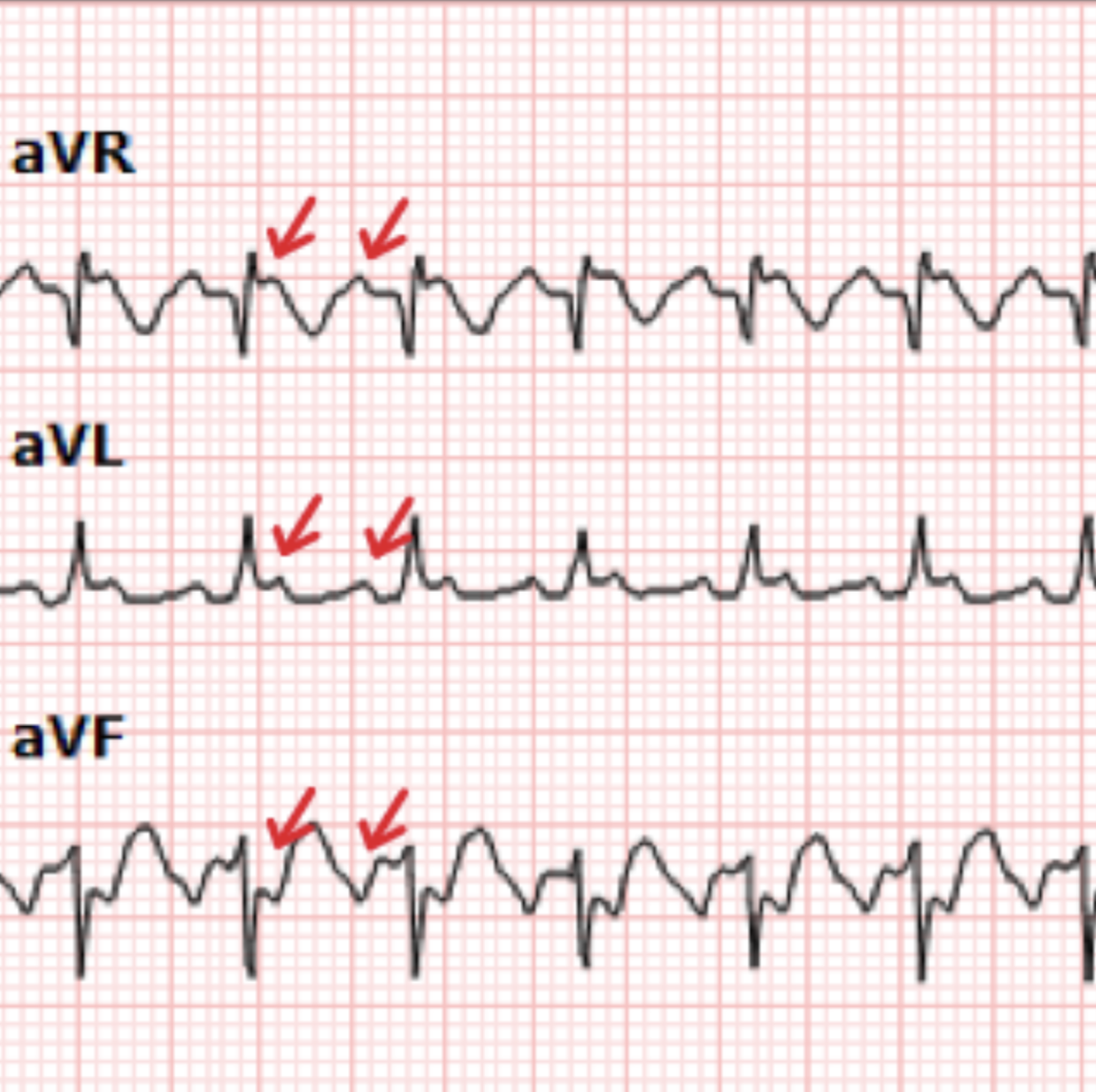
Figure 5. Image depicting flutter waves (red arrow) from the EKG in Figure 2
However, in a 1:1 or 2:1 block, it can be very difficult to pick out these small sawtooth elements. Like in this patient it can be difficult to identify flutter waves when they are inverted in inferior leads. This is why you may have to rely on other clues such as lack of an isoelectic baseline, regularity of the heart rate (a 2:1 block will very consistently show a persistent, unchanging rate of 150), and patient history. Adenosine can be a good tool to slow down the heart rate to obtain a closer look at the underlying rhythm as well, which was helpful in this case. Adenosine will not stop the arrhythmia because adenosine acts on the AV node. As we saw in this patient, adenosine temporarily ceases conduction of the flutter waves to the ventricles, dramatically slowing or even briefly stopping QRS complexes altogether. This reveals a brief run of rapid sawtooth P waves and alerts the clinician to the true underlying rhythm.
Ultimately, these patients will require rate control with Calcium Channel Blockers, Beta Blockers, or, in some cases, Digoxin. Our patient ended up requiring a diltiazem drip for rate control and was ultimately discharged on diltiazem PO. If patients are unresponsive to medications, they may require ablation. Finally, similar to patients with atrial fibrillation, the CHADS2-VASC may be used to stratify need for anticoagulation.
Take Home Points:
Atrial Flutter is one of the most common types of SVT and can have many causes, but most commonly are secondary to pulmonary disease.
While the EKG may not always show the classic “sawtooth” pattern that you were taught in medical school, there are other clues to look for, such as a fixed rate of 150 and lack of an isoelectric baseline.
First line treatment is going to be calcium channel blockers, however some patient may require multiple agents or even ablation to ultimately achieve rate control.
References:
Rodriguez Ziccardi M, Goyal A, Maani CV. Atrial Flutter. [Updated 2022 Dec 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK540985/
Burns, Ed. Buttner, R. Atrial Flutter. Life in the Fast Lane. October 8, 2024. Atrial Flutter • LITFL • ECG Library Diagnosis
Rush Emergency Medicine. Image: Atrial Flutter AV Blocks. October 7, 2018. Blog Post, Available at: https://rushem.org/atrial-flutter-av-blocks/
Authored by Veronica Gonzalez MD, Michael Hohl MD, Erica Dolph MD, Abish Kharel MD, & Ari Edelheit MD