
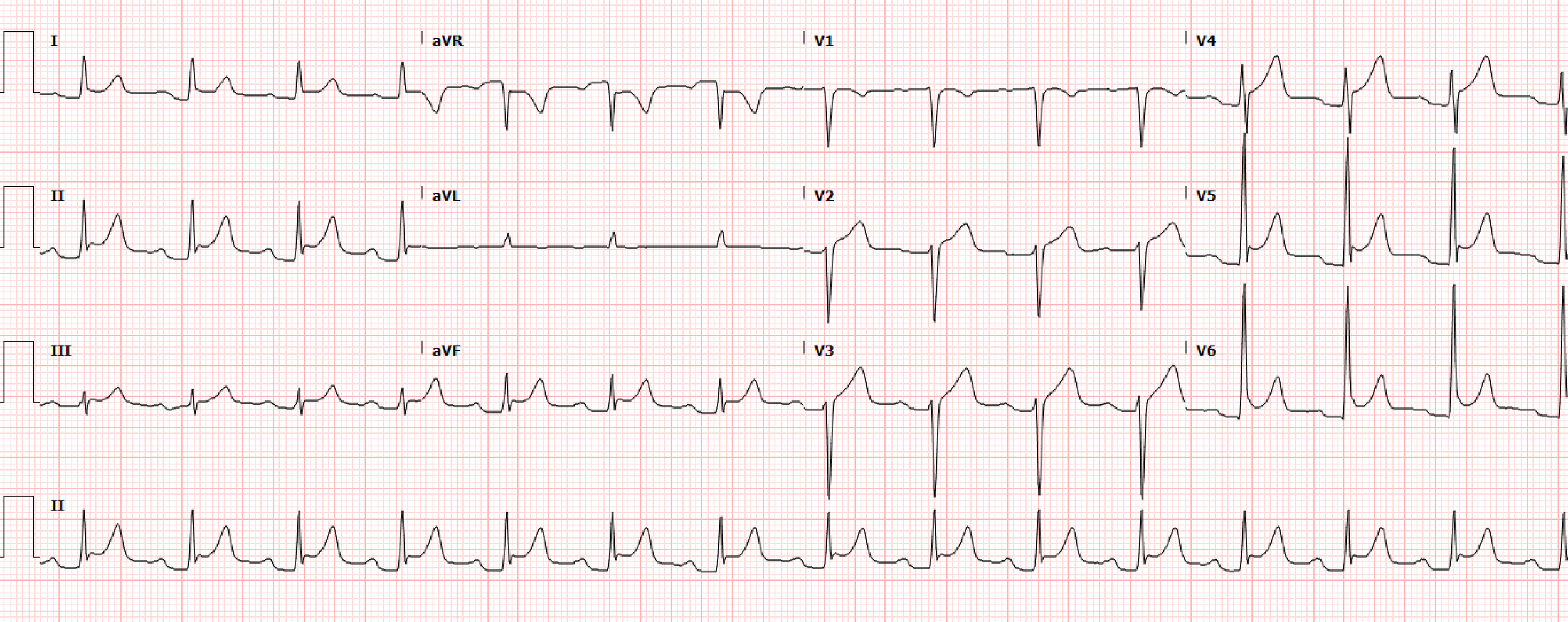
44-year-old otherwise healthy male presents to the emergency department with chest pain. The pain started yesterday mid-day and is described as central and substernal with radiation across the chest and up into the throat. The patient also reports shortness of breath worse with deep breathing and exertion. The patient is incarcerated but otherwise has no historical risk factors for tuberculosis, pulmonary embolism, or cardiac disease. An EKG (Figure 1) is obtained.
Interpretation: Rate: 86 bpm; Rhythm: normal sinus; Axis: normal axis (I: pos., II: pos., aVF: pos); Intervals: PR: 230, prolonged; QRS: 97, normal; QT: 384, normal; P-Waves: normal morphology; QRS Complex: normal, good R wave progression; ST Segment/T-waves: diffuse 1mV ST elevation from baseline; PR Segment: diffuse 1mV PR depression from baseline
A focused cardiac ultrasound is performed which shows normal ED, no pericardial effusion, and no region wall motion abnormalities. The labs are significant for an undetectable troponin, normal chemistry, normal white count, and a positive d-dimer of 0.6 ng/dL.
What is your differential for the above EKG? What additional tests might you consider?
Discussion
The ED ordered a CT pulmonary angiography with the elevated d-dimer which showed no evidence of acute pulmonary embolism to the lobar level and was otherwise unremarkable. The patient was ultimately diagnosed with pericarditis with documentation stating “that patient met 2/4 criteria" and discharged on high dose NSAIDs for treatment.
These criteria are:
Retrosternal, positional, pleuritic chest pain often alleviated by sitting forward and exacerbated by lying flat
High pitched cardiac friction rub bet her at left lower sternal border
EKG changes as described below
Echocardiogram demonstrating pericardial effusion [1].
This patient’s EKG (Figure 1) demonstrates diffuse 1mV ST elevations in nearly all leads except for aVL (poor quality lead), aVR (appropriate ST depression), and V1. This can be seen in Benign Early Repolarization (BER), Left Ventricular Hypertrophy (LVH), Left Bundle Branch Block (LBBB), Ventricular Aneurysm, Hyperkalemia, Pericarditis, and Takotsubo Cardiomyopathy [2]. Notably, even with this diffuse elevation, the EKG (Figure 1) does not meet traditional STEMI criteria. Severe triple vessel disease or high coronary occlusion (OMI criteria) could result in diffuse ST elevation but would show ST elevation in aVR, rather than ST depression.
The EKG (Figure 1) also demonstrates diffuse 1mV PR depression which has a much narrower differential of Pericarditis or Atrial Ischemia [3]. Rarely, PR depression can be observed in massive pulmonary embolism with right atrial strain, however it is typically accompanied by ST elevations including elevation in aVR and other signs of right heart strain (T-wave inversion in inferolateral leads) [4].
One study showed that the combination of PR depression in both precordial and limb leads was able to differentiate pericarditis from acute OMI (positive 96.7% and negative power 90%) [5]. Additional EKG findings that help support the diagnosis of acute pericarditis include:
Saddle-shaped ST elevation (lead V6 in Figure 1) affecting leads across multiple coronary distributions
Reciprocal changes in aVR seen as PR elevation and ST depression (present in Figure 1)
Spodick’s Sign seen as downsloping TP segment (lead II in Figure 1) [6].
Within the clinical context of this patient, the only overlapping diagnosis on the differential is acute pericarditis, and with all of the EKG findings listed about this is the leading diagnosis. So what about the positive d-dimer and the possibility of acute pulmonary embolism?
It is important to remember that the d-dimer itself is an inflammatory marker not simply a “rule out” test for acute pulmonary embolism and can be elevated in COVID-19, coagulopathies, pneumonia, and often in pericarditis. Studies show age-adjusted d-dimer positivity in 50-75% of cases of acute pericarditis [7-8]. A proposed biomarker algorithm for assisting in the work-up and diagnosis of pericarditis was proposed by Mascolo et al. (Figure 2).
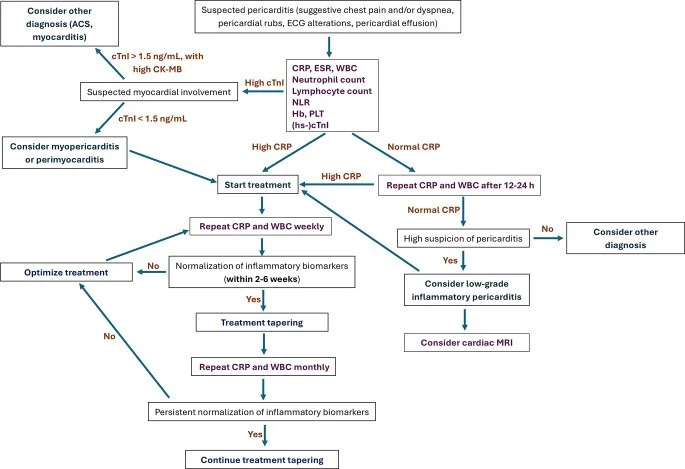
Figure 2. Pathway for suspected pericarditis
Take Away Points
Diffuse PR Depressions + ST Elevations + Reciprocal Changes in aVR highly suggest the diagnosis of acute pericarditis
Pleuritic chest pain and an elevated D-dimer are common in acute pericarditis
Patient must meet 2 of the 4 criteria to be clinically diagnosed with pericarditis → 1) Chest Pain, 2) Cardiac Friction Rub, 3) EKG Changes, 4) Pericardial Effusion
References
Khandaker MH, Espinosa RE, Nishimura RA, et al. Pericardial disease: diagnosis and management. Mayo Clin Proc. 2010;85(6):572-593. doi:10.4065/mcp.2010.0046
Francis BR, Arshad N, El-Din M, Antoun I. ST Elevation in aVR: An Atypical Presentation of Pulmonary Embolism. Clin Case Rep. 2025;13(8):e70671. Published 2025 Jul 29. doi:10.1002/ccr3.70671
Porela P, Kytö V, Nikus K, Eskola M, Airaksinen KE. PR depression is useful in the differential diagnosis of myopericarditis and ST elevation myocardial infarction. Ann Noninvasive Electrocardiol. 2012;17(2):141-145. doi:10.1111/j.1542-474X.2012.00489.x
Lazaros G, Vlachakis PK, Theofilis P, et al. D-dimer as a diagnostic and prognostic plasma biomarker in patients with a first episode of acute pericarditis. Eur J Intern Med. 2023;116:58-64. doi:10.1016/j.ejim.2023.06.017
Mascolo R, Bizzi E, Martelli M, et al. Old and New Biomarkers in Idiopathic Recurrent Acute Pericarditis (IRAP): Prognosis and Outcomes. Curr Cardiol Rep. 2025;27(1):17. Published 2025 Jan 11. doi:10.1007/s11886-024-02170-y
Authored by Michael Hohl MD and Ari Edelheit MD