
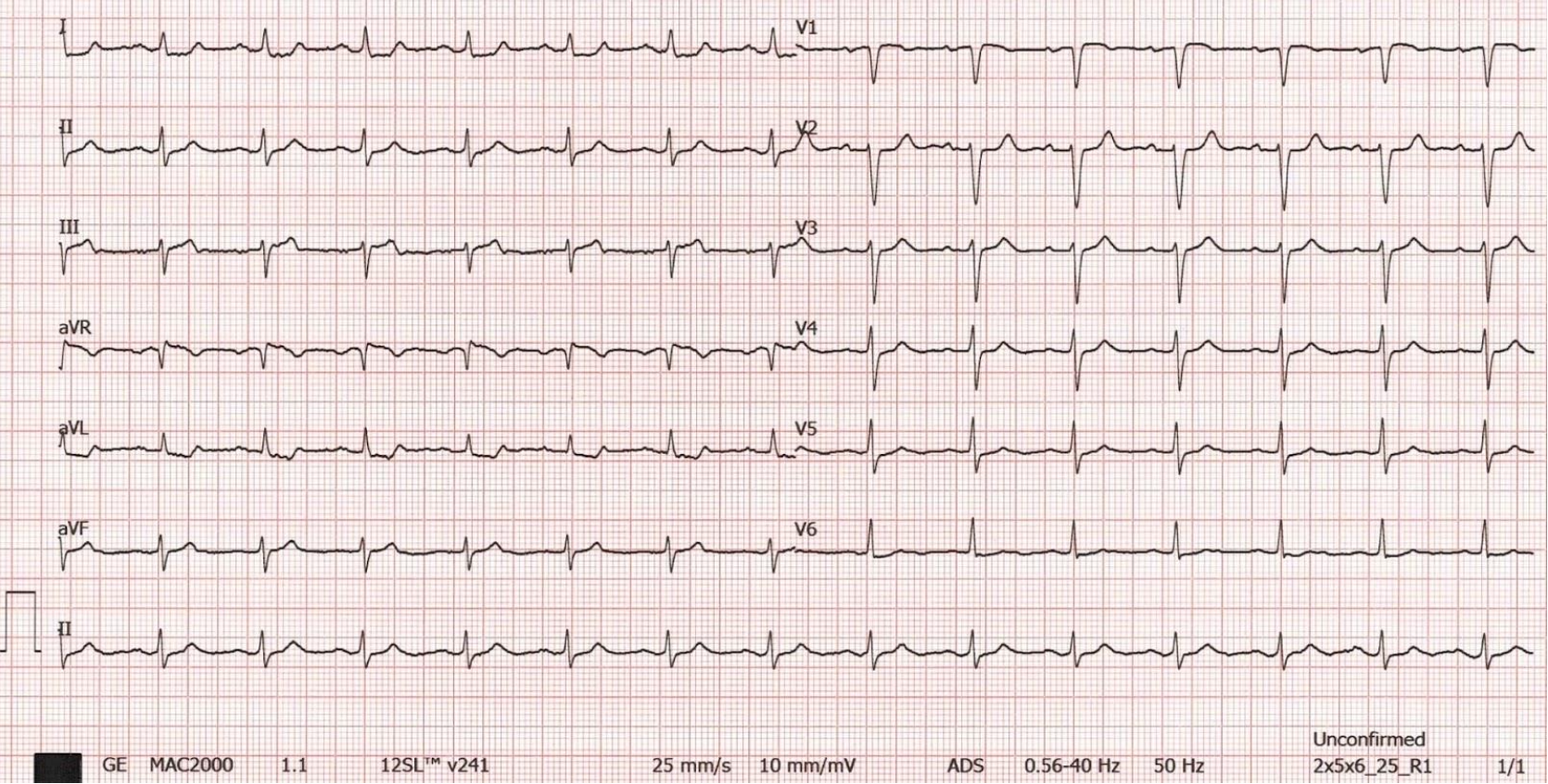
A 57-year-old female with a past medical history of hypertension presents to the emergency department (ED) with the complaint of chest pain that started just prior to arrival. The patient has no other complaints. An ECG is obtained (Figure 1).
Interpretation:
Rate: 90 bpm; Rhythm: normal sinus rhythm; Axis: normal axis (I: pos., II: pos., aVF: eqv.) Intervals: PR: 120, normal; QRS: 90, normal; QT: 400, normal; P-Waves: present; QRS Complex: normal, delayed R wave progression; ST Segment/T-waves: 1mV ST elevation in lead III, 0.5mV elevation in lead V1, 1mm reciprocal ST depression in lead I, aVL, 0.5 mV progressing to 1 mV depression in leads V4-V6, and non-specific inverted/biphasic T- waves in leads aVL, V1, upright/biphasic T-wave in III
The cath lab was activated. The patient was found to have a right coronary artery (RCA) occlusion (Figure 2), and a stent was placed. The patient was admitted to the Cardiac ICU post-stent placement.

Figure 2. RCA occlusion (Centre de Cardiologie Interventionnelle Belledonne: https://ccibelledonne.com/en/patient-guide/coronary-angiography/).
Discussion:
In 2020, Aslanger et al. reviewed ECG and angiography findings of 1,000 patients experiencing a non-ST elevation myocardial infarction (NSTEMI) and 1,000 control patients not experiencing an NSTEMI and found that the specific Aslanger pattern was observed in 6.3% of NSTEMI patients. It was found to be a predictor of a larger infarct size and had a five time increase in-hospital mortality when not diagnosed promptly.
The Aslanger pattern is a specific ECG pattern that is concerning for acute inferior occlusion myocardial infarction (OMI) with multi-vessel disease and allows the detection of inferior myocardial infarction that does not show ST-elevation or fulfill STEMI criteria. This pattern predicts left circumflex (LCx) or right coronary artery (RCA) acute coronary occlusion despite ST elevation in only lead III (and often V1).
In 2023, Miyauchi et al. looked at whether the Aslanger pattern was useful not only for diagnosis, but also for predicting hemodynamic collapse and a poor prognosis. The study identified a total of 48% of patients with non-STEMI had the Aslanger pattern. In addition, 80% of patients with the Aslanger pattern had multi-vessel disease, 30% required the use of mechanical circulatory support, and 20% had in-hospital mortality.
However, there are also limitations to the Aslanger pattern. It was found to be present in 0.5% of patients without acute ischemia, which could have resulted from previous ischemic events. A similar pattern could occur in acute inferior OMIs when in the presence of previous infarctions.
So what exactly are the criteria of the Aslanger pattern?
Inferior ST elevation isolated to lead III
Concomitant ST depression in any of V4-V6, with a positive/terminally positive T-wave
ST segment in V1 > V2

Figure 3. Aslanger pattern as identified on ECG (ECG Weekly: https://ecgweekly.com/weekly-workout/st-segment-elevation-not-contiguous/).
Does the Aslanger pattern warrant a cath lab activation?
In a 2022 expert consensus article for chest pain disposition in the Emergency Department, the American College of Cardiology (ACC) endorsed acute reperfusion therapy (catheterization or thrombolytics) not only for STEMI but also for left bundle branch block or ventricular paced rhythm with Sgarbossa criteria or with Smith-modified Sgarbossa criteria, de Winter T waves, non-ST-elevation-acute coronary syndrome (NSTE-ACS) with refractory angina, hemodynamic or electrical instability, developing heart failure. They did not endorse acute reperfusion therapy for Aslanger pattern.
However, in 2023 in the Journal of Catheterization and Cardiovascular Interventions endorsed the same criteria as the ACC but also pushed for reperfusion therapy for Aslanger pattern. Therefore, if you see this pattern on an ECG in a patient with concerning ACS symptoms, you should consider emergently consulting cardiology for further guidance.
Take Away Points:
Beware ST elevation in leads III + V1.
Aslanger pattern has a high likelihood of acute coronary occlusion involving RCA or LCx.
Recognition of the Aslanger pattern should prompt an emergent cardiology consultation.
Authored by Taylor Wahrenbrock, MD; Michael Hohl, MD; and Ari Edelheit, MD.
References:
Aslanger E, Yıldırımtürk Ö, Şimşek B, Sungur A, Türer Cabbar A, Bozbeyoğlu E, Karabay CY, Smith SW, Değertekin M. A new electrocardiographic pattern indicating inferior myocardial infarction. J Electrocardiol. 2020 Jul-Aug;61:41-46.
Miyauchi E, Kuwazuru K, Arikawa R, et al. Clinical Features of the Aslanger Pattern to Compensate for the Limitation of ST-Elevation Myocardial Infarction (STEMI) Criteria. Cureus. 2023;15(1):e33227. Published 2023 Jan 1. doi:10.7759/cureus.33227
Kontos, M, de Lemos, J. et al. 2022 ACC Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department: A Report of the American College of Cardiology Solution Set Oversight Committee. JACC. 2022 Nov, 80 (20) 1925–1960. https://doi.org/10.1016/j.jacc.2022.08.750
Zoni CR, Mukherjee D, Gulati M. Proposed new classification for acute coronary syndrome: Acute coronary syndrome requiring immediate reperfusion. Catheter Cardiovasc Interv. 2023;101(7):1177-1181. doi:10.1002/ccd.30667