

A 30-year-old male with a past medical history of Wolff-Parkinson-White Syndrome (WPW) s/p ablation (2023), HIV on highly active antiretroviral therapy (HAART), and seizure disorder presents to emergency department for palpitations and left-sided chest pain that started a few hours prior to arrival. The patient denies any recent systemic infectious symptoms, drug use, travel, or chronic medication non-adherence. An initial ECG was obtained in triage (Figure 1).
Interpretation:
Rate: 206 bpm; Rhythm: regular narrow complex tachycardia; Axis: right axis deviation (I: neg, II: pos., aVF: pos) Intervals: PR: n/a, no p-waves; QRS: 90, normal; QT: 344, normal; P-Waves: no p-wave preceding QRS, retrograde p-waves (lead V1, aVR); QRS Complex: good R wave progression; ST Segment/T-waves: inverted T-waves in leads II, III, aVF, aVR
The patient was diagnosed with WPW with orthodromic atrioventricular reentrant tachycardia (AVRT) involving a posteroseptal accessory pathway in consultation with Cardiac Electrophysiology (EP), to whom the patient was previously known. The decision was made to give an initial dose of procainamide 100mg IV, and the heart rate decreased from low 200s bpm to 180s bpm, but did not terminate the AVRT. An additional dose of procainamide 100mg IV was administered, which resulted in a decrease in the patient’s blood pressure to 90s/60s, but no termination of the AVRT. Subsequently, adenosine 6mg IV was administered, which resulted in conversion to normal sinus rhythm. EP recommended admission to the general medical floor with telemetry and inpatient cardiac electrophysiology consultation.
Discussion:
AVRTs are a subtype of supraventricular tachycardia that occurs when an anatomic accessory pathway exists between the atrial and ventricular conduction systems. Two subtypes exist, orthodromic and antidromic, which appear different on ECG and have different treatments. Careful ECG interpretation and medication selection is necessary for proper management.
Orthodromic AVRT:
Antegrade (forward) conduction through the AV node and returns to atria retrograde via an accessory pathway
Normal QRS < 120 ms
Heart rate typically 200-300 bpm
Retrograde P-waves with a long PR interval (>70 ms)
Treatment is targeted toward the AV node [1]

Figure 2. Orthodromic AVRT. Adapted from https://ecgwaves.com/topic/pre-excitation-avrt-wolff-parkinson-white-wpw-syndrome/.
Antidromic AVRT:
Antegrade conduction from the atria through the accessory pathway and returns retrograde (backward) conduction through the AV node
Wide QRS > 120 ms
Heart rate typically 200-300 bpm
P-waves rarely seen
Treatment is targeted toward the accessory pathway [1]
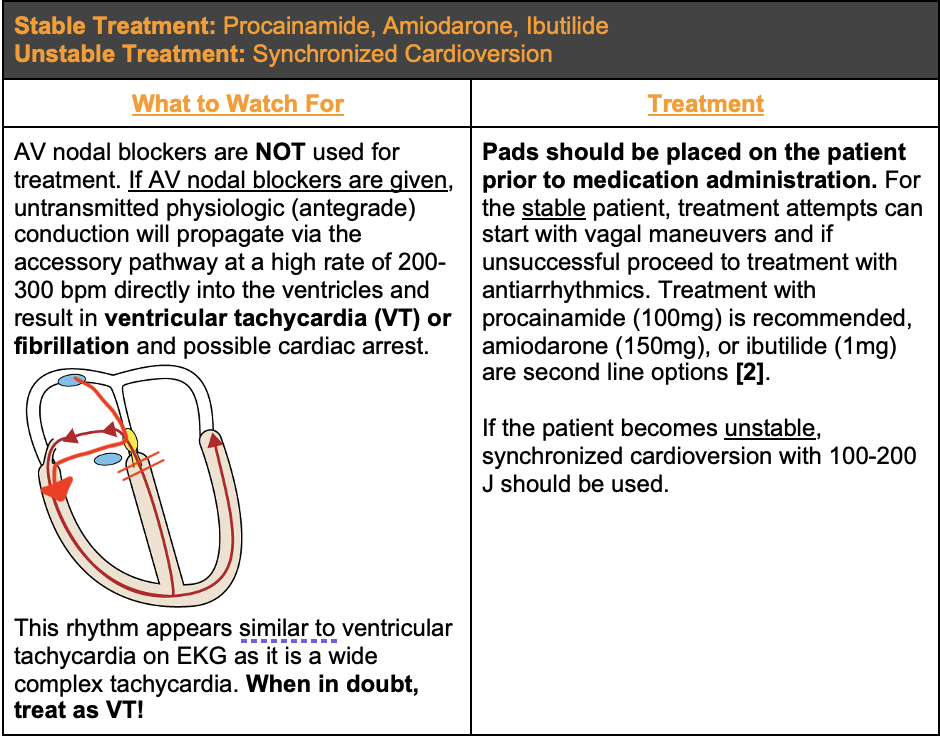
Figure 3. Antidromic AVRT. Adapted from https://ecgwaves.com/topic/pre-excitation-avrt-wolff-parkinson-white-wpw-syndrome/.
Despite having orthodromic AVRT, the patient in this case was given procainamide as a first line medication by EP. Two reasons may exist for this decision:
There is evidence that procainamide might be a good treatment option for both antegrade and retrograde AVRT [3], and
Procainamide is a frequently used and safe medication in patients with underlying WPW with tachyarrhythmias [4].
Take Away Points:
If you can’t differentiate antidromic AVRT from ventricular tachycardia, always treat as ventricular tachycardia.
It seems reasonable to give procainamide to all patients with AVRT, however AV nodal blockers may be more effective for orthodromic AVRT (especially if resistant to procainamide).
Do not give AV nodal blockers to antidromic AVRT, as you may precipitate ventricular tachycardia, fibrillation, and/or cardiac arrest
All unstable AVRT need electricity. Use synchronized cardioversion starting at 100-200 J.
Authored by Michael Hohl, MD.
References:
Buttner, R. (2022, May 19). Atrioventricular re-entry tachycardia (AVRT). Life in the Fast Lane. https://litfl.com/atrioventricular-re-entry-tachycardia-avrt/
Page, R. L., Joglar, J. A., Caldwell, M. A., Calkins, H., Conti, J. B., Deal, B. J., Estes, N. A. M., Field, M. E., Goldberger, Z. D., Hammill, S. C., Indik, J. H., Lindsay, B. D., Olshansky, B., Russo, A. M., Shen, W.-K., Tracy, C. M., & Al-Khatib, S. M. (2016). 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia. Circulation, 133(14). https://doi.org/10.1161/cir.0000000000000311.
Leitch, J, Klein, G, Yee, R. et al. Differential effect of intravenous procainamide on anterograde and retrograde accessory pathway refractoriness. JACC. 1992 Jan, 19 (1) 118–124.https://doi.org/10.1016/0735-1097(92)90061-Q.
Mandel, W. J., Laks, M. M., Obayashi, K., Hayakawa, H., & Daley, W. (1975b). The Wolff-Parkinson-White Syndrome: Pharmacologic effects of procaine amide. American Heart Journal, 90(6), 744–754. https://doi.org/10.1016/0002-8703(75)90464-0.